April 2020
|
April 2020 // Volume 58 // Number 2 // Research In Brief // v58-2rb2



Parent-Focused Childhood Obesity Intervention Improves Family Functioning and Children's Well-Being
Abstract
An Extension-implemented parent-focused childhood obesity intervention designed to improve family functioning around healthful eating and exercise was evaluated. Thirty-six parents and their children, aged 5–13, were randomized to a 12-week intervention condition or control condition. Intervention parents, compared to control group parents, felt more confident in promoting children's healthful eating and exercise, worried less about their children's weight, and engaged in fewer counterproductive parenting behaviors. The children of these parents, as compared to children of control group parents, lost weight and displayed better social-emotional functioning. These results highlight Extension's important role in disseminating evidence-based childhood obesity interventions.
Extension has great potential for disseminating high-quality health promotion programs, including interventions focused on reducing childhood obesity. Extension educators have a good understanding of evidence-based practice, including implementation fidelity, and generally strong relations with schools and community agencies serving children and families (Spoth, Guyll, Lillehoj, Redmond, & Greenberg, 2007). As a result, Extension represents a promising avenue for promoting childhood obesity prevention in community settings (Gunter, Nader, Armington, Hicks, & John, 2017; Lanigan & Power, 2008). We evaluated the success of Extension educators, working in conjunction with school personnel, in implementing an adapted evidence-based intervention focused on childhood obesity.
Childhood Obesity
Childhood obesity is a significant public health problem that affects one in six children in the United States (Ogden et al., 2016). Childhood obesity is associated with many physical health problems, including cardiovascular diseases and type 2 diabetes (Deckelbaum & Williams, 2001).
Childhood obesity is also associated with a wide range of social-emotional problems, such as anxiety, depression, and peer rejection/victimization (Barlow, 2007; Vila et al., 2004). Moreover, when children are overweight, they are more likely to have food tantrums or refuse to engage in physical activity (Walsh Pierce & Wardle, 1997; West & Sanders, 2009). These challenges are compounded by ineffective parenting, such as permissive practices (e.g., not monitoring or setting rules for healthful eating and physical activity) or coercive practices (e.g., pressuring the child to eat or overly restricting foods), which are associated with even more social-emotional problems and a greater risk for unhealthful eating habits (Birch & Fisher, 2000; Vereecken, Keukelier, & Maes, 2004)
A key childhood obesity prevention strategy is promoting healthful lifestyle behaviors, which include dietary and physical activity patterns (Davison & Birch, 2001). When parents have confidence and knowledge about healthful lifestyles and use effective parenting practices to manage their children's lifestyle behaviors, children tend to eat more healthful food and engage in more physical activity (Faith, Scanlon, Birch, Francis, & Sherry, 2004; Golan & Weizman, 2001).
Lifestyle Triple P
The Lifestyle Positive Parenting Program, also known as Lifestyle Triple P (LTP) (West & Sanders, 2010), is a variant of Triple P (Sanders, 1999). LTP is an evidence-based parenting program originally developed and evaluated in Australia. LTP aims to promote children's positive behaviors and well-being by increasing parents' knowledge of healthful lifestyle behaviors and decreasing their use of ineffective practices. Importantly, LTP aims to improve children's behavior in general and their behavior around food and exercise in particular (Sanders, Markie-Dadds, Tully, & Bor, 2000).
Only two published trials of LTP exist to date, showing promising results for Australian families (West, Sanders, Cleghorn, & Davies, 2010) and Dutch families (Gerards et al., 2015) when implemented in clinical settings. Both trials demonstrated changes in parents' perceived self-efficacy for promoting healthful lifestyle behaviors, and both trials demonstrated improvements in children's healthful lifestyle behaviors. West et al. (2010) also found reductions in children's body mass index.
Objectives
We implemented and evaluated the first trial of LTP in the United States, which also was the first trial of LTP in a community rather than clinical setting. The study was the result of a collaboration across our team of university researchers, Pennsylvania State University Extension educators, and local school district personnel.
The objectives of the intervention were as follows:
- to improve parents' confidence and parenting practices around managing children's lifestyle behaviors,
- to reduce children's excess body weight, and
- to improve overweight and obese children's social-emotional functioning.
Method
The study was approved by the institutional review board of Pennsylvania State University.
Sample
Our study included 48 mothers or other female caregivers (no fathers chose to participate) and their elementary school–aged children, aged 5–13, 61% of whom were girls. Herein we refer collectively to the mothers and female caregivers who participated as parents. About 64% of the families were White, 30% were Black, 3% were Asian, and 3% were Latinx. Twenty-two percent of parents were single, 67% had completed some professional training or college, and most reported yearly income in the $20,000–$50,000 range.
Extension educators recruited parents from local public elementary schools via flyers, social media, and school nurse and local doctor referrals of families with children who were overweight or obese. Parents were told that the program was focused on healthful lifestyle behaviors.
Parents and one target child per family were initially randomized to receive LTP, n = 27, or be placed in the waiting list control condition, n = 21. Twenty-one families in the LTP group and 15 in the control group completed the baseline assessments and were included in the study.
Procedure
Pennsylvania State University Extension educators and school personnel cofacilitated each LTP group. Employees of Triple P America conducted the official training in LTP, which included a review of the family systems and social learning theory underpinnings of the intervention but focused on practice and certification in implementing the standardized curriculum with fidelity. Our research team, the Extension educators, and the school personnel collaborated with the LTP program developer to adapt LTP so that it was more appropriate for families in our communities. Details of that process are reported in the companion Ideas at Work report in this issue of Journal of Extension (DiNallo et al., 2020).
Our version of LTP lasted 12 weeks and consisted of ten 90-min weekly group sessions and two 20-min individual phone calls delivered to the parents. Group sessions included up to 10 parents and were offered in the evening at local elementary schools. The group sessions focused on promoting lifestyle behaviors, such as eating healthful foods and exercising, as well as general parenting practices, such as setting reasonable limits and delivering effective, nonharsh consequences. We provided travel vouchers, childcare, and meals to encourage participation. In the individual structured phone calls, the LTP facilitators reviewed progress with parents and addressed barriers they encountered in trying to implement new skills.
At the end of LTP, parents completed process evaluations of program acceptability and feasibility (see appendix). The average rating of intervention quality was 6.63 (SD = .74), near the maximum score of 7. The average rating of intervention content and materials was 6.00 (SD = 1.22) out of 7. The average rating of meeting family needs was 6.24 (SD = .99) out of 7. In responses to open-ended questions about ways to improve the intervention, the most common suggestion was to include children in intervention activities.
Measures
Assessments were conducted at baseline and immediately after the intervention (see appendix). Also at baseline, parents answered questions about basic family demographics, including family medical problems, which can be signs of risk for obesity.
Parents' confidence in their abilities to manage children's healthful lifestyle behaviors was assessed with the Lifestyle Behaviour Checklist (West & Sanders, 2009), which includes 25 items (e.g., "How confident are you in successfully dealing with your child's eating of unhealthy snacks?"), rated on a Likert scale of 1 = not at all confident to 9 = completely confident (α = .97). Parents' concern about their children's weight was assessed with the Child Feeding Questionnaire (Birch et al., 2001), which includes three items (e.g., "How concerned are you about your child's eating too much when you are not around?"), rated on a 5-point Likert scale of 1 = unconcerned to 5 = very concerned (α = .80). Parents' lax and overreactive behaviors when interacting with their children were assessed with the Parenting Scale (Arnold, O'Leary, Wolff, & Acker, 1993), which includes five items on lax parenting (e.g., "When my child does something I don't like, I do something about it every time it happens" versus "I often let it go") and five items on overreactive parenting (e.g., "When my child misbehaves, I raise my voice and yell" versus "I speak to my child calmly"), rated from 1 to 7, depending on which anchor parents think is more accurate (α = .83 and .82, respectively).
Children's height and weight were measured by trained school nurses using standardized equipment and following standardized procedures (Lohman, Roche, & Martorell, 1988). Age- and sex-specific body mass index (BMI) z-scores (zBMI) were calculated according to Centers for Disease Control and Prevention growth charts (Kuczmarski et al., 2002).
Children's behavior was assessed with the parent-rated Strengths and Difficulties Questionnaire (Goodman, 2001), which was applicable for the age group in the study and includes five items on prosocial behavior (e.g., "Considerate of other people's feelings"), five items on conduct problems (e.g., "Often lies or cheats"), five items on emotional symptoms (e.g., "Often unhappy, depressed, or tearful"), and 5 items on peer problems (e.g., "Picked on or bullied by other children"), rated from 0 = not true to 2 = certainly true (α = .84, .65, .67, and .69, respectively).
Data Analysis
Linear regression equations were estimated for each outcome. Independent variables in each equation included intervention condition (1 = intervention, 0 = control), baseline assessment of the outcome, study site, school, child age, child sex, family income, and number of family medical problems. Results are reported as intervention effect sizes, or Cohen's d (Cohen, 1988), which represent the difference between the intervention and control group means divided by the sample standard deviation and adjusted for model covariates: .20 = a small effect size, .50 = a medium effect size, .80 = a large effect size, and 1.20 = a very large effect size. We used probability values of less than .05 to establish statistical significance. We applied multiple imputation (averaged across 50 imputed data sets) to reduce any bias associated with missing data (Schafer, 1997).
Results
Figure 1 shows the flow of participants through the study. There were no baseline differences in study outcomes. In addition, no baseline characteristics were significantly related to study attrition.
Figure 1.
Flow of Families Through Study
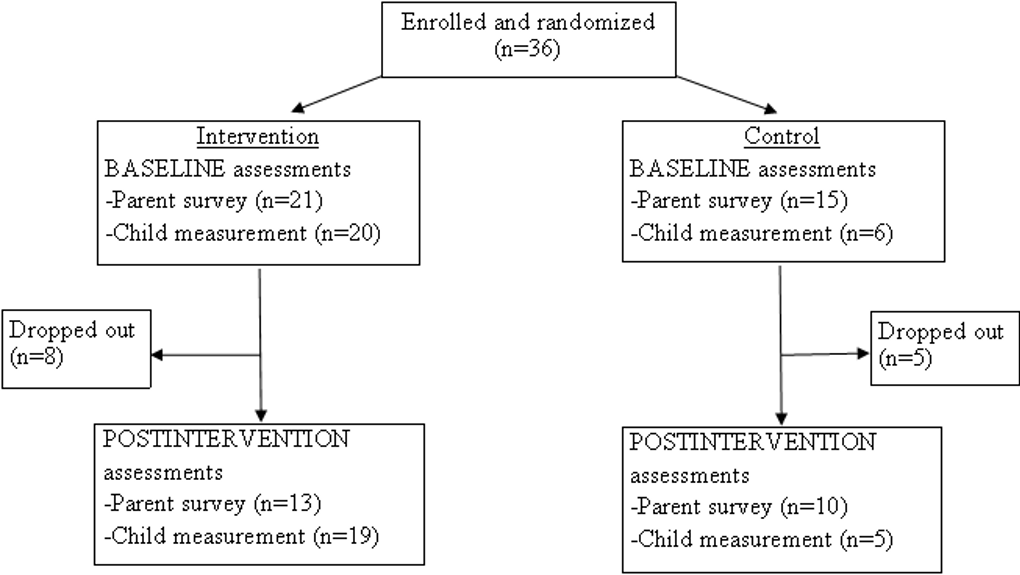
Table 1 shows imputed means at baseline and following the intervention and intervention effect sizes. LTP parents, compared to control group parents, experienced significantly improved confidence in their ability to manage children's healthful lifestyle behaviors, d = 1.22, p < .001. This effect size represents a very large difference of almost one-and-one-quarter standard deviations in means for the two groups of parents. LTP parents, compared to control group parents, also reported fewer concerns about children's weight, d = (−.80), p < .01, a large intervention effect. There was no group difference in lax parenting; however, LTP parents were less likely than control group parents to engage in overreactive behaviors, d = (−.79), p < .05, a large intervention effect.
When parents were assigned to participate in LTP instead of the control group, their children had a lower body mass index, d = (−30), p < .10, at the end of the 12-week intervention period, a small to medium intervention effect at a trend level.
When parents were assigned to participate in LTP instead of the control group, their children displayed more prosocial behaviors, d = .49, p < .05, a medium intervention effect, and fewer conduct problems, d = (−.74), p < .05, a large intervention effect.
| Measure | LTP | Waiting list control | Intervention effect Cohen's d | ||
|---|---|---|---|---|---|
| Baseline | Postintervention | Baseline | Postintervention | ||
| Parent outcomes | |||||
| Confidence in abilities to manage child's lifestyle behaviorsa | 166.11 | 191.59 | 133.65 | 185.70 | 1.22*** |
| Concern about child weightb | 3.62 | 3.01 | 3.76 | 3.18 | -.80** |
| Lax parenting practicesc | 2.65 | 2.61 | 3.33 | 3.24 | -0.24 |
| Overreactive parenting practicesc | 3.44 | 3.14 | 3.71 | 3.00 | -0.79* |
| Child outcomes | |||||
| Body size (zBMI) | 1.81 | 1.77 | 2.12 | 2.29 | -.30† |
| Prosocial behaviorsd | 8.33 | 8.21 | 8.20 | 7.25 | .49* |
| Conduct problemsd | 3.29 | 2.77 | 2.70 | 4.02 | -.74* |
| Emotional problemsd | 2.57 | 2.77 | 2.93 | 3.74 | -.38 |
| Peer problemsd | 4.76 | 4.18 | 4.50 | 5.25 | -.35 |
|
Note. LTP = Lifestyle Triple P. zBMI = body mass index z-score. Missing data: 8% for parent measures, 27% for child body size.
aLifestyle Behaviour Checklist (West & Sanders, 2009); highest possible confidence score = 225. bChild Feeding Questionnaire (Birch et al., 2001); scale is 1 = unconcerned to 5 = very concerned. cParenting Scale (Arnold, O'Leary, Wolff, & Acker, 1993); scale of 1—7, with higher scores indicating more lax or more overreactive parenting practices. dStrengths and Difficulties Questionnaire (Goodman, 2001); scores range from 0 to 10, with higher score indicating the presence of more prosocial behaviors, conduct problems, emotional problems, or peer problems. †p < .10. *p < .05. **p < .01. ***p < .001. |
|||||
Discussion
We evaluated a parent-based childhood obesity intervention program delivered through Extension and adapted for community settings in the United States. Similar to previous trials of LTP (Gerards et al., 2015; West et al., 2010), our study showed large improvements in parents' confidence in their ability to manage children's healthful lifestyle behaviors, which may positively affect children's health (Davison & Birch, 2001; West et al., 2010). Perhaps as a result of that increase in confidence, parents reported feeling less concerned and anxious about children's weight. Parents who participated in LTP also reported being less overreactive in the way they set limits and encouraged children's positive behaviors.
Consistent with the findings from a previous trial of LTP in a very different setting (West et al., 2010), we found a small to medium intervention and control group difference (p < .10) in children's BMI in just 12 weeks. Given how difficult it is to lose weight, this finding is highly encouraging.
We also found that there were improvements in children's prosocial behaviors and conduct problems when parents participated in LTP. These improvements might be the result of positive changes in parenting practices. The improvements also might be the result of adopting more healthful lifestyles.
The strengths of the study include use of an evidence-based intervention tested with an experimental design in community settings. The limitations include a small sample size and attrition over time.
Implications for Extension
Our study demonstrated that Extension educators working in their communities can replicate the positive results of LTP from previous trials in clinical settings. The study adds to the growing body of research suggesting that interventions targeting parents may be a promising way to promote optimal health in children. As important, our study highlights how Extension can be an important venue for disseminating such interventions.
Acknowledgments
The study presented was funded by the National Center for Advancing Translational Sciences, grant UL Tr000127, to the Clinical and Translational Science Institute of Pennsylvania State University, the U.S. Department of Agriculture Childhood Obesity Prevention Training Program, grant 2011-67001-30117, and the National Institute of Diabetes and Digestive and Kidney Diseases, grant F31DK109578. The authors declare they have no conflict of interest.
References
Arnold, D. S., O'Leary, S. G., Wolff, L. S., & Acker, M. M. (1993). The Parenting Scale: A measure of dysfunctional parenting in discipline situations. Psychological Assessment, 5, 137–144.
Barlow, S. E. (2007). Expert committee recommendations regarding the prevention, assessment, and treatment of child and adolescent overweight and obesity: Summary report. Pediatrics, 120(Suppl. 4), S164–192. doi:10.1542/peds.2007-2329C
Birch, L. L., & Fisher, J. O. (2000). Mothers' child-feeding practices influence daughters' eating and weight. The American Journal of Clinical Nutrition, 71(5), 1054.
Birch, L. L., Fisher, J. O., Grimm-Thomas, K., Markey, C. N., Sawyer, R., & Johnson, S. L. (2001). Confirmatory factor analysis of the Child Feeding Questionnaire: A measure of parental attitudes, beliefs and practices about child feeding and obesity proneness. Appetite, 36, 201–210.
Cohen, J. (1988). Statistical power analyses for the behavioral sciences (2nd ed.). Hillsdale, NJ: Lauwrence Erlbaum Associates.
Davison, K. K., & Birch, L. L. (2001). Childhood overweight: A contextual model and recommendations for future research. Obesity Reviews, 2(3), 159–171. doi:10.1046/j.1467-789x.2001.00036.x
Deckelbaum, R. J., & Williams, C. L. (2001). Childhood obesity: The health issue. Obesity Reviews, 9(Suppl. 4), 239S–243S. doi:10.1038/oby.2001.125
DiNallo, J. M., Welsh, J. A., Li, J. C., & Nix, R. L. (2020). Cultural and contextual adaptation of a childhood obesity prevention intervention program. Journal of Extension, 58(2), Article v58-2iw2. Available at: https://joe.org/joe/2020april/iw2.php
Faith, M. S., Scanlon, K. S., Birch, L. L., Francis, L. A., & Sherry, B. (2004). Parent-child feeding strategies and their relationships to child eating and weight status. Obesity Reviews, 12, 1711–1722.
Gerards, S. M., Dagnelie, P. C., Gubbels, J. S., van Buuren, S., Hamers, F. J., Jansen, M. W., . . . Kremers, S. P. (2015). The effectiveness of Lifestyle Triple P in the Netherlands: A randomized controlled trial. PLoS One, 10(4), e0122240. doi:10.1371/journal.pone.0122240
Golan, M., & Weizman, A. (2001). Familial approach to the treatment of childhood obesity: Conceptual model. Journal of Nutrition Education, 33(2), 102–107.
Goodman, R. (2001). Psychometric properties of the Strengths and Difficulties Questionnaire. Journal of the American Academy of Child & Adolescent Psychiatry, 40(11), 1337–1345. doi:10.1097/00004583-200111000-00015
Gunter, K. B., Nader, P. A., Armington, A., Hicks, J. C., & John, D. (2017). Evaluation of an Extension-delivered resource for accelerating progress in childhood obesity prevention: The BEPA-Toolkit. Journal of Extension, 55(2), Article v55-2a5. Available at: https://joe.org/joe/2017april/a5.php
Kuczmarski, R. J., Ogden, C. L., Guo, S. S., Grummer-Strawn, L. M., Flegal, K. M., Mei, Z., . . . Johnson, C. L. (2002). 2000 CDC growth charts for the United States: Methods and development. Vital and Health Statistics, 11(246), 1–190.
Lanigan, J., & Power, T. G. (2008). Obesity prevention and health promotion: How family life educators view their role. Journal of Extension, 46(6), Article 6FEA5. Available at: https://www.joe.org/joe/2008december/a5.php
Lohman, T. G., Roche, A. F., & Martorell, M. (1988). Anthropometric standardization reference manual. Champaign, IL: Human Kinetics.
Ogden, C. L., Carroll, M. D., Lawman, H. G., Fryar, C. D., Kruszon-Moran, D. K., Kit, B. K., & Flegal, K. M (2016). Trends in obesity prevalence among children and adolescents in the United States, 1988–1994 through 2013–2014. JAMA, 315(21), 2292–2299. doi:10.1001/jama.2016.6361
Sanders, M. R. (1999). Triple P-Positive Parenting Program: Towards an empirically validated multilevel parenting and family support strategy for the prevention of behavior and emotional problems in children. Clinical Child and Family Psychology Review, 2(2), 71–90.
Sanders, M. R., Markie-Dadds, C., Tully, L. A., & Bor, W. (2000). The Triple P-Positive Parenting Program: A comparison of enhanced, standard, and self-directed behavioral family intervention for parents of children with early onset conduct problems. Journal of Consulting and Clinical Psychology, 68(4), 624–640.
Schafer, J. L. (1997). Analysis of incomplete multivariate data. London, UK: Chapman and Hall/CRC Press.
Spoth, R. L., Guyll, M., Lillehoj, C. J., Redmond, C., & Greenberg, M. T. (2007). Prosper study of evidence‐based intervention implementation quality by community–university partnerships. Journal of Community Psychology, 35(8), 981–999. doi:10.1002/jcop.20207
Vereecken, C. A., Keukelier, E., & Maes, L. (2004). Influence of mother's educational level on food parenting practices and food habits of young children. Appetite, 43(1), 93–103. doi:10.1016/j.appet.2004.04.002
Vila, G., Zipper, E., Dabbas, M., Bertrand, C., Robert, J. J., Ricour, C., & Mouren-Simeoni, M. C. (2004). Mental disorders in obese children and adolescents. Psychosomatic Medicine, 66(3), 387–394.
Walsh Pierce, J., & Wardle, J. (1997). Cause and effect beliefs and self-esteem of overweight children. Journal of Child Psychology and Psychiatry, 38(6), 645.
West, F., & Sanders, M. R. (2009). The Lifestyle Behaviour Checklist: A measure of weight-related problem behaviour in obese children. International Journal of Pediatric Obesity, 4(4), 266–273. doi:10.3109/17477160902811199
West, F., & Sanders, M. R. (2010). Facilitator's manual for group Lifestyle Triple P. Milton QLD, Australia: Triple P International Pty. Ltd.
West, F., Sanders, M. R., Cleghorn, G. J., & Davies, P. S. (2010). Randomised clinical trial of a family-based lifestyle intervention for childhood obesity involving parents as the exclusive agents of change. Behaviour Research and Therapy, 48(12), 1170–1179. doi:10.1016/j.brat.2010.08.008
Appendix
Table of Measures Used in Study
| Measure | Concept(s) assessed |
|---|---|
| Parent outcomes | |
| Family Demographic Background (West & Sanders, 2010) | Demographic information, family health history |
| The Lifestyle Behaviour Checklist (West & Sanders, 2009) | Parents' confidence in dealing with children's lifestyle behaviors, extent of children's lifestyle behaviors |
| Child Feeding Questionnaire (Birch et al. 2001) | Parents' concerns about children's weight |
| The Parenting Scale (Arnold, O'Leary, Wolff, & Acker, 1993) | General parenting behaviors such as laxness and overreactivity |
| Child outcomes | |
| The Strengths and Difficulties Questionnaire (Goodman, 1997) | General child behaviors such as prosocial behaviors, conduct problems, emotional problems, and peer problems |
| Body mass index z-score | Body size and risks for obesity |
| Process measures | |
| Family Satisfaction Questionnaire | Whether the program met families' needs, the impact the program had on their parenting skills and their children's behavior, and their satisfaction with the group leaders, program format, and program content |
| Participant Post-Study Evaluation Survey | Additional feedback about the recruitment process, curriculum, and implementation of the various components of the program |