June
2012
|
June 2012 // Volume 50 // Number 3 // Feature // v50 -3a5



Extension Newsletters and Individual Counseling: Equally Effective in Changing Worksite Wellness Participants Dietary Intakes
Abstract
The
Affordable Care Act provides impetus for Extension efforts in
worksite wellness. The study reported here examined the
influence of two worksite wellness interventions, newsletters and
individual counseling. Surveys examined dietary and physical activity
behaviors of participants pre- and post-intervention (N=157).
Descriptive statistics, paired samples t-tests, and
repeated measures ANOVA identified change in nutrient intakes;
McNemar's Test evaluated physical activity participation. Both
interventions significantly increased fruit/vegetable
servings, vitamin C, potassium, magnesium, and dietary fiber while
decreasing total fat, saturated fat, percent fat, and dietary
cholesterol. There is opportunity for Extension in worksite wellness
programming and research to strengthen evidence-based practice.
Introduction
Cardiovascular disease (CVD) remains the leading cause of death in the United States (US) (Jones et al., 2009) and cost $475.3 billion in 2009 (American Heart Association, 2009). Overweight and obesity are significant risk factors for CVD. Collectively, these chronic conditions present a significant cost to employers through healthcare claims and lost workdays. Maintaining a healthy body weight, consuming recommended amounts of fruits and vegetables, and exercising regularly have been identified as steps adults can take to reduce risk for CVD (Centers for Disease Control and Prevention [CDC], 2007).
Fruit and vegetable consumption increases intake of potassium and dietary fiber, which lowers CVD risk (Bazzano et al., 2001; Ludwig et al., 1999). The 2005 Dietary Guidelines for Americans (DGA) recommend individuals following a 2,000-calorie diet consume two cups of fruit and two and one-half cups of vegetables daily (US Department of Health and Human Services [US DHHS] and US Department of Agriculture, 2005). Most individuals do not meet recommended intakes of fruits and vegetables (Guenther, Dodd, Reedy, & Krebs-Smith, 2006). Between 1988 and 2006, individuals eating five or more servings (two and one-half cups) of fruits and vegetables a day decreased from 42% to 26% (King, Mainous, Carnemolla, & Everett, 2009).
Physical activity (PA) guidelines released October 2008 provide absolute, relative, and practical guidelines that parallel the DGA (US DHHS, 2008). Absolute guidelines state "adults should accumulate 500-1000 MET minutes of physical activity a week," whereas relative guidelines state "adults should perform at least 150 minutes a week of moderate intensity aerobic activity or 75 minutes a week of vigorous-intensity aerobic PA or an equivalent combination of moderate and vigorous intensity aerobic activity." Individuals meeting PA recommendations vary relative to the PA criterion; however, Behavioral Risk Factor Surveillance System data (CDC, 2007) and National Health Interview Survey (NHIS) data (CDC, 2010) suggest that less than half of all adults meet PA recommendations. Between 1988 and 2006, those performing PA at least 12 times per month decreased by 10% (King, Mainous, Carnemolla, & Everett, 2009).
The Task Force for the Community Guide (CDC) reported worksite wellness programs improved dietary fat intake, blood cholesterol, blood pressure, PA, and number of days lost from work due to illness or disability (Task Force Community Services, 2007). A major worksite goal for Healthy People 2010 was ≥75% of worksites offer a comprehensive health promotion program (US DHHS, 2000).
Worksite wellness can be offered in a variety of modes, including print materials, Internet, face-to-face education, and telephone. A 1-month PA intervention delivered via print material was shown to help employees improve their PA (Griggin-Blake & DeJoy, 2006). Unfortunately, a similar study reported no significant improvement in participants meeting PA recommendations despite increased PA (Marshall, Leslie, Bauman, Marcus, & Owen, 2003).
Research suggests print nutrition education materials were read and saved more often, and evaluated more favorably, among participants than CD-ROM-delivered material (Kroeze, Oenema, Campbell, & Brug, 2008). Yet nutrition education via interactive-tailored CD-ROM and print materials resulted in similar, significant reductions in total fat and energy intake (Kroeze, Oenema, Campbell, & Brug, 2008a). Nutrition education delivered by registered dietitians (RDs) at the worksite has also been shown to improve the health status of individuals (Hunt, Hilgenkamp, & Farley, 2000). Abood and colleagues (2003) reported decreased energy intake, total fat intake, saturated fat intake, and cholesterol intake with individual counseling.
Improvement in health outcomes and high returns on investment (ROI) make worksite wellness programming worth a company's time and money. A ROI of $3.48 for every dollar spent on worksite wellness (Aldana, 2001) has been suggested; others report a 25% reduction in healthcare and absenteeism costs (Chapman, 2003). Despite the high ROI, worksites continue to look for the most-cost effective method of providing wellness programming to employees.
The purpose of the study reported here was to examine two modes of worksite wellness programming, print newsletters and individual counseling, on health behaviors. Fruit and vegetable intake, estimated nutrient intakes, and physical activity were examined pre- and post-intervention.
Methods
Design
Participants either received eight newsletters, published by the Extension service of a Midwestern university, or individual counseling with a RD three times (2 hours total) over a 16-week period. Both groups completed pre- and post-intervention surveys [Block Food Frequency screener (Block, Gillespie, Rosenbaum, & Jenson, 2000)] salt survey, and NHIS Adult Health Behaviors PA questions (NHIS, 2008). Participants were given and signed an informed consent document describing their rights as research participants and describing the research project prior to participation. All protocols followed during the study were approved by the university's Human Subjects Review Board.
Participants
Newsletters
Six small businesses in a Midwestern state were identified and contacted by their health insurance carrier. Selected businesses had higher healthcare or prescription claims related to high blood pressure. Extension program specialists promoted and explained the newsletter program to employees at each worksite. Participants (N=112) from each of the six worksites were an employee or spouse of an employee at the worksite; females were not pregnant.
Individual Counseling
Employees from a Midwestern university were recruited to participate in an existing employee benefit—three individual sessions with an RD. Participants were recruited via list of employees interested in counseling sessions, new employee orientation sessions, and university/college electronic and hard-copy newsletters. Participants (N=49) were employees of the university; females were not pregnant.
Intervention
Newsletters
Participants received the first of eight bi-weekly newsletters after completing the pre-intervention survey; subsequent issues were distributed by the employer. Newsletters were based upon the Dietary Approaches to Stop Hypertension (DASH) diet, which focuses on a diet low in saturated fat, cholesterol, and total fat and increased fruits, vegetables, and fat-free or low-fat dairy products (US DHHS, 2006). An overview of the nutrition and PA topics in the newsletters appears in Table 1. Incentives corresponded to newsletter topics and included pedometers, stretch bands, and calendars. Sixteen weeks after receiving the first newsletter, participants completed the post-survey.
| Nutrition | Physical Activity(PA) | |
| Issue 1 |
|
|
| Issue 2 |
|
|
| Issue 3 |
|
|
| Issue 4 |
|
|
| Issue 5 |
|
|
| Issue 6 |
|
|
| Issue 7 |
|
|
| Issue 8 |
|
|
Individual Counseling
RDs providing individual counseling included a university wellness program employee and a graduate student. Participants returned completed pre-surveys, which had been emailed, at the first session with the RD.
The first counseling session lasted 45 minutes to 1 hour, while the second and third sessions were approximately 30 minutes each. The second and third sessions were scheduled 3 to 4 weeks after the first and second visits, respectively. Primary topics discussed by the RDs were MyPyramid, snacks, exercise, portion control, and increasing fruit and vegetable intake. Many participants expressed interest in weight loss; however, this topic was not discussed directly by the RDs; rather healthful eating was promoted. Incentives for participation were the same as for the newsletters (pedometer, stretch band, calendar).
Approximately 16 weeks after the first session (4 weeks after the third visit), participants completed the post-survey. Subjects completing all three sessions as well as the post-survey were also eligible to participate in a free healthy cooking demonstration.
Measures: Pre/Post Intervention Surveys
The Block Food Frequency screener is a validated and reliable tool providing fruit/vegetable and meat/snack scores (Block, Gillespie, Rosenbaum, & Jenson, 2000). The fruit/vegetable score, not including beans/legumes, predicts fruit and vegetable servings, whereas the fruit/vegetable score, including beans/legumes, predicts vitamin C, magnesium, potassium, and dietary fiber intakes. The meat/snack score predicts total fat, saturated fat, percent fat, and dietary cholesterol intakes.
PA was examined using five PA questions from the 2008 NHIS (NHIS, 2008). Participants' self-reported PA was categorized as meeting or not meeting the 2008 PA and MSA guidelines (US DHHS, 2008).
Currently, there are no validated tools to estimate salt or sodium intake due to the wide variability of sodium in products at restaurants and grocery store shelves and prepared at home. A five-question survey, similar to the Block Food Frequency screener, was created to examine change in consumption of high salt/sodium foods pre- to post-intervention. The salt score reflects frequency consuming of high salt/sodium foods, not predicted salt or sodium intake; higher scores suggest more frequent consumption.
Statistical Analysis
Statistical analysis was performed using SPSS for Windows (v17.0; Chicago, IL). Descriptive statistics and paired samples t-tests explored demographic variables and pre-/post-intervention nutrient intakes. Change in participant nutrient intakes pre- and post-intervention was examined by paired samples t-tests and repeated measures ANOVA. Non-parametric statistics (McNemar's Test) were used to examine PA relative to 2008 PA recommendations. Two participant subgroups (two worksites [same company] receiving newsletters and participants receiving individual counseling) were selected to evaluate the two interventions using independent samples t-test, Pearson's chi-square test, and repeated measures ANOVA. The level of statistical significance for all analyses was set at p<0.05.
Results
A total of 157 participants (N=112 newsletter, N=45 counseling) completed the worksite wellness interventions. Age and gender distribution of the participants appear in Table 2.
| Newsletter (N=112) | Counseling (N=45) | |
| Males | ||
| 21-35 | 25 (51.02%) | 1 (16.67%) |
| 36-50 | 17 (34.69%) | 1 (16.67%) |
| 51-65 | 7 (14.29%) | 4 (66.67%) |
| 66+ | 0 (0.00%) | 0 (0.00%) |
| Females | ||
| 21-35 | 20 (31.75%) | 5 (12.82%) |
| 36-50 | 24 (38.10%) | 15 (38.46%) |
| 51-65 | 14 (22.22%) | 19 (48.72%) |
| 66+ | 5 (7.94%) | 0 (0.00%) |
Results of paired samples t-tests for estimated nutrient intakes appear in Table 3. Sample size varied on specific variables due to incomplete data on some surveys. Fruit/vegetable servings and fruit/vegetable score nutrients (fiber, potassium, magnesium, vitamin C) increased significantly among all participants (p<0.05). Meat/snack score nutrients (total fat, saturated fat, percent fat, and cholesterol) decreased significantly among all participants (p<0.05). Further examination revealed the significant increases in nutrient intake occurred in males, whereas the significant decreases occurred in females. Salt score decreased significantly among all participants (p<0.05), primarily among males. No significant change was seen in participants meeting any of the PA guidelines.
| Variable | Males(N=55)
x̄ ±SD |
Females (N=102)
x̄ ±SD |
Total (N=157)
x̄ ±SD |
|||
| Pre | Post | Pre | Post | Pre | Post | |
| Fruit/vegetable servingsa | 3.94±1.61 | 4.48±1.46* | 4.05±1.64 | 4.20±1.61 | 4.01±1.62 | 4.31±1.55* |
| Fruit/vegetable scoreb | ||||||
| Fiber (gm) | 18.35±4.86 | 20.08±4.45* | 13.97±4.91 | 14.20±4.91 | 15.63±5.21 | 16.43±5.52* |
| Potassium (gm) | 3.58±0.70 | 3.84±0.61* | 3.02±0.70 | 3.06±0.71 | 3.23±0.75 | 3.36±0.78* |
| Magnesium (mg) | 385.18±71.53 | 411.46±63.26* | 310.39±70.71 | 314.08±72.48 | 338.78±79.59 | 351.04±83.64* |
| Vitamin C (mg) | 140.28±40.40 | 155.38±34.25* | 128.09±40.87 | 130.35±41.10 | 132.72±40.98 | 139.85±40.40* |
| Meat/snack scorec | ||||||
| Total fat (gm) | 86.99±16.04 | 84.44±16.76 | 90.14±17.30 | 85.95±15.32* | 88.92±16.83 | 85.36±15.85* |
| Saturated fat (gm) | 29.31±5.88 | 28.37±6.14 | 22.85±6.34 | 21.32±5.62* | 25.35±6.91 | 24.05±6.75* |
| Percent fat (%) | 33.37±4.01 | 32.74±4.19 | 33.66±4.33 | 32.61±3.83* | 33.55±4.19 | 32.66±3.96* |
| Cholesterol (mg) | 297.90±53.17 | 289.63±53.42 | 216.09±55.71 | 202.46±49.56* | 247.80±67.64 | 236.25±66.39* |
| Salt scored | 4.98±2.66 | 3.68±2.33* | 3.88±2.48 | 3.71±2.43 | 4.33±2.60 | 3.70±2.38* |
| Meeting PA guidelines | ||||||
| PA (%)e | 72.1 | 79.1 | 65.0 | 73.8 | 67.5 | 75.6 |
| MSA(%)f | 46.8 | 53.2 | 32.2 | 38.9 | 37.2 | 43.8 |
| PA and MSA(%)g | 44.2 | 48.8 | 28.2 | 34.6 | 33.9 | 39.7 |
|
*significant difference pre/post (p<0.05) |
||||||
Repeated measures ANOVA, where age was entered as a covariate and gender and mode of intervention as independent variables, examined change in dietary intakes. Fruit and vegetable servings increased significantly from pre- to post-intervention (data not shown; p<0.05) with subsequent increases in estimated nutrient intakes of vitamin C, magnesium, potassium and fiber (Figure 1a). Total fat, saturated fat, percent fat, and dietary cholesterol also decreased significantly (Figure 1b). A small-to-moderate effect size was observed for all nutrients (Figure 1a and 1b). No significant change was noted from pre- to post-intervention for salt score (data not shown).
Figure 1.
Change in Nutrient Intake Among Participants
a) Change in vitamin C, magnesium, dietary fiber, and potassium intake among males (N=52) and females (N=85)
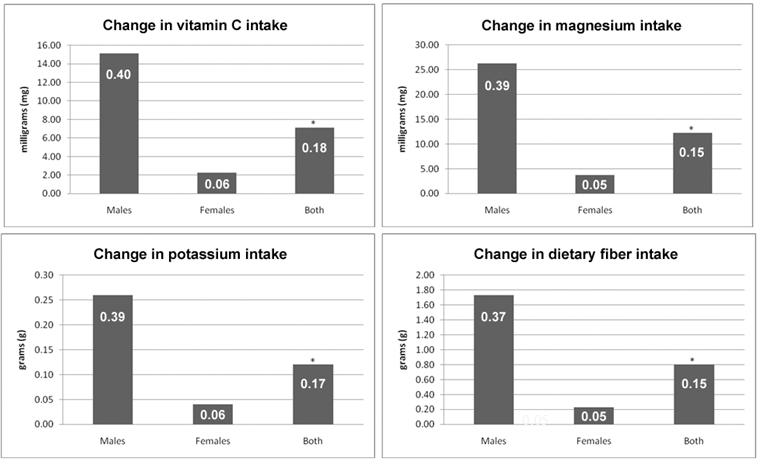
b) Change in total fat, saturated fat, percent fat, and dietary cholesterol intake among males (N=50) and females (N=79)
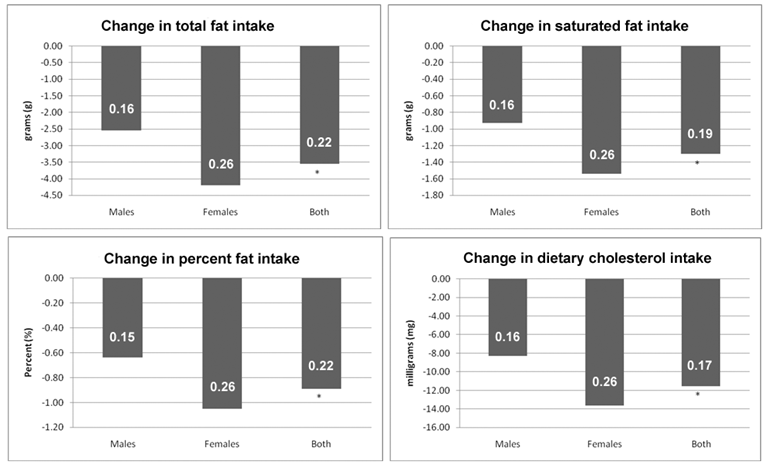
*significant change in nutrient (p-value<0.05) Effect size shown on bars in white
Results suggest that age and gender predict select estimated nutrient intakes. Age was a significant predictor (p<0.05) of fruit/vegetable servings and dietary fiber intake; fruit/vegetable servings increased, while dietary fiber intake decreased with age. Male gender predicted higher intakes of potassium, magnesium, and dietary fiber (p<0.05). Conversely, female gender predicted lower intakes of saturated fat and dietary cholesterol, but a higher total fat intake (p<0.05).
Age was also a significant predictor (p<0.05) of change in estimated fruit/vegetable servings as well as change in potassium, magnesium, and dietary fiber intakes. Intakes of these nutrients were less likely to change with age.
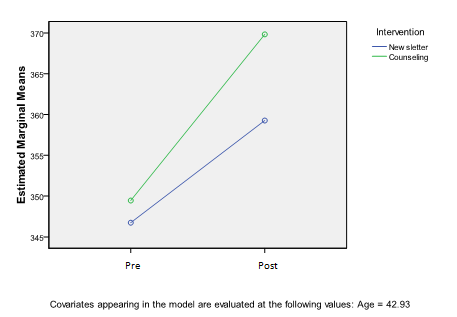
Plots of estimated marginal means for specific nutrient intakes pre- to post-intervention by intervention appear in Figure 2. Visual examination of the slopes suggests a difference between the interventions. It appears the newsletter intervention may be more effective in decreasing cholesterol intake, whereas individual counseling may be more effective in increasing the magnesium intake. This prompted further examination of the data by intervention. Selection of a subgroup among newsletter participants was necessary due to demographic differences between participants receiving newsletters or individual counseling. Two worksites (same company) receiving newsletters were selected for the comparison. The subgroup of the newsletter intervention and university participants was predominantly high school- to college-educated employees performing white collar job descriptions.
Figure 2.
Pre- and
Post-Intervention Estimated Marginal Means by Intervention
a)Estimated marginal means of cholesterol intake (mg)
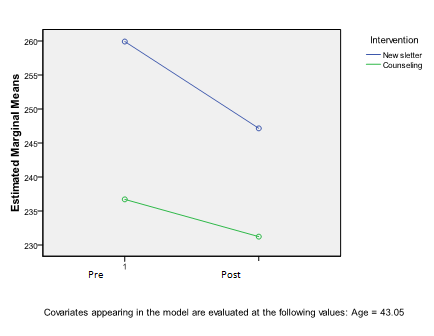
b)Estimated marginal means of magnesium intake (mg)
Age was entered as a covariate and gender and intervention as independent variables in a repeated measures ANOVA model to examine change in nutrient intakes by intervention. Fruit and vegetable servings increased as a result of the interventions, but there was no significant difference between interventions (data not shown). Fruit/vegetable score nutrients (Figure 3a) significantly increased, and meat/snack score nutrients (Figure 3b) significantly decreased among all participants; however, no difference was seen between interventions. A small-to-moderate effect size was observed for all nutrients (Figure 3a and 3b).
Figure 3.
Change in Nutrient Intake by Intervention
a) Change in vitamin C, magnesium, potassium, and dietary fiber by intervention (newsletters N=31; counseling N=43)
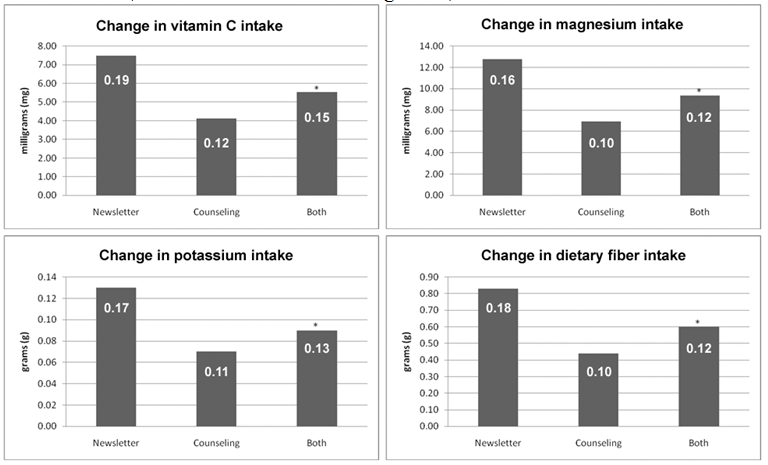
b) Change in total fat, saturated fat, percent fat, and dietary cholesterol by intervention (newsletters N=28; counseling N=36)
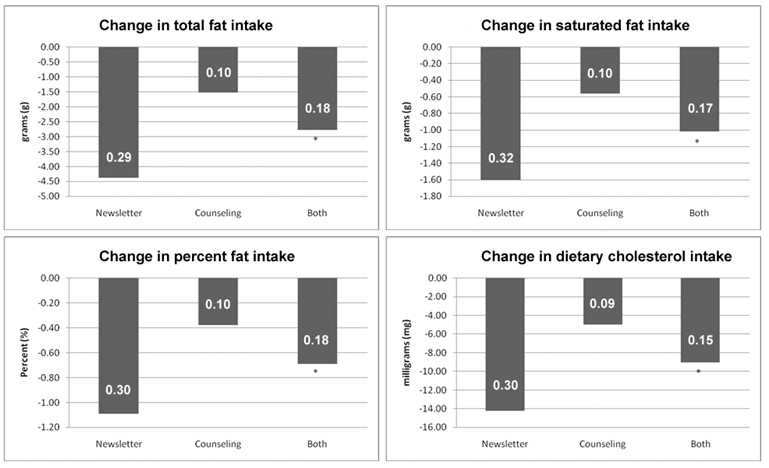
*significant change in nutrient (p-value<0.05)
Effect size shown on bars in white
In summary, results suggest fruit and vegetable servings, including predicted vitamin C, potassium, magnesium, and dietary fiber intakes, significantly increased, while predicted total fat, saturated fat, percent fat, and dietary cholesterol intakes significantly decreased between pre- and post-worksite intervention. While some changes were gender-specific, they were not intervention-specific. The salt score decreased significantly (p<0.05) according to the paired sample t-test between pre- and post-worksite intervention, but when age, sex, and intervention were entered into the repeated measures ANOVA model, no difference was observed. These results suggest both newsletters and individual counseling can be effective in changing dietary intakes; however, neither method was more effective than the other.
Discussion
Positive change in health behaviors (fruit/vegetable intake and physical activity) have been reported with Extension programs in worksite and community settings using friendly team competition (Case, 2010; Litchfield et al., 2007). The study reported here examined two other types of worksite wellness intervention, print newsletters and individual counseling. Results suggest both newsletters and individual counseling improved dietary intake, which is consistent with previous studies (Kroeze et al., 2008; Kroeze, et al., 2008a; Abood, Black, & Feral, 2003; Brown & Olson, 1988). However, neither intervention significantly increased those meeting PA guidelines, also consistent with previous studies (Marshall et al., 2003).
Participants (average age 49.3 years; 88% female) receiving individual counseling experienced significant decreases (p<.05) in total fat, saturated fat, and dietary cholesterol (repeated measures ANOVA with age and gender as moderators). These results are similar to those reported by another program (average age 34.3 years; 96% female) (Abood, Black, & Feral, 2003). It is interesting that similar results were found despite notable differences in the amount of time participants spent in individual counseling (2 hours over 16 weeks versus 8 hours over 8 weeks).
Decreases in total fat, saturated fat, and dietary cholesterol intakes (p<.05) were also observed among newsletter recipients (repeated measures ANOVA with age and gender as moderators) (average age 40.4 years; 61% female). This is similar to a previous study, where recipients of tailored print-material (average age 43.4 years; 55% female) experienced significant decreases in total fat, saturated fat, and energy intake; however, no significant change was observed with generic print-material (Kroeze et al., 2008a).
Print materials have been shown to improve PA; recipients of stage-matched or standard PA print materials increased their PA similarly (Griffin-Blake & DeJoy, 2006). Participants receiving PA print materials with bi-weekly reinforcement letters significantly improved PA; however, no significant improvement in meeting 1996 CDC PA recommendations occurred (Marshall et al., 2003). CDC recommendations for PA in 1996 stated adults should accumulate 30 minutes moderate intensity PA on most, if not all, days of the week, similar to the current recommendation of 150 minutes of moderate intensity PA per week (US DHHS, 2008). Participants meeting PA guidelines in this study improved from pre- and post-intervention, but not significantly.
Results of the study reported here suggest both newsletters and individual counseling were effective in improving nutrient intakes, with neither being more effective than the other. Age was predictive of estimated fruit/vegetable servings and dietary fiber, whereas gender predicted estimated potassium, magnesium, dietary fiber, total fat, saturated fat, and dietary cholesterol intakes. As age increased, estimated fruit/vegetable servings increased, but dietary fiber intake decreased. It is possible that while older participants made a concerted effort to increase fruit/vegetable servings, they decreased intake of other sources of fiber (i.e., grains) to compensate. Male gender predicted higher estimated intakes of potassium, magnesium, and dietary fiber. Conversely, being female predicted lower estimated intakes of saturated fat and dietary cholesterol, but higher total fat. It appears males were more successful increasing intakes, whereas women were more successful restricting intakes. No significant difference in the amount of change in intake by gender was observed.
Age significantly predicted change in estimated fruit/vegetable servings and estimated intakes of potassium, magnesium, and dietary fiber intakes. With age estimated change in intakes decreased. It is likely that decreasing caloric needs with age decreases total food intake, decreasing the amount of change possible.
Worksite wellness programs benefit both the employee and employer. Poor employee health has been linked to higher direct healthcare costs, disability rates, absenteeism, workers' compensation, and rates of injury as well as lower work output (Partnership for Prevention, 2005). Improved health outcomes and high ROI make a worksite wellness program worth a company's time and money. A review of worksite wellness programs suggests a savings to cost ratio of $3.50 to $1.00 from reduced absenteeism and health care costs (Aldana, 2001), some even suggest a $6.00 to $1.00 (Berry, Mirabito, & Baun, 2010).
Both print newsletters and individual counseling with an RD in the study reported here influenced nutrient intake of employees; however, the more cost effective method would be newsletters. The cost for implementing the newsletter intervention in the study was approximately one-tenth that of individual counseling. The cost of newsletters would be higher if developed and customized by the individual employer; however, a number of agencies/organizations including Extension provide such materials.
Limitations and Implications for Extension
While the findings of the research suggest opportunities for Extension programming in worksite wellness, limitations do exist. First, the study included participants who self-selected, which suggests predisposition to making behavior change. Results would likely be different if participants were randomly selected. Second, all surveys were self-report, which can be skewed by respondents anticipating desired responses. Third, participant education and income levels were not available, which compromised comparison of the interventions. For the comparison, a subgroup of those receiving the newsletter was selected to more closely mirror the university population receiving individual counseling. Census information revealed the mean income of the counties of these worksites locations were similar (US Census Bureau, 2008). Finally, although the study did not include control groups for comparison, previous studies have demonstrated interventions are significantly more effective in changing behavior relative to controls (Mills, Kessler, Cooper & Sullivan, 2007; Sternfeld & Block, 2009; Sorensen et al., 1998).
Worksite wellness was identified as opportunity for Extension programming 20 years ago (Blase, 1992) and remains an untapped opportunity. The Affordable Care Act is impetus for effective, efficient preventive healthcare, including worksite wellness. Extension is well positioned to support further research and programming relative to nutrition, health, and wellness (Case, 2010) in this new era of preventive healthcare. This is particularly true in rural areas, typically underserved by the traditional healthcare system. The Affordable Care Act promotes affordable and accessible wellness and prevention services by requiring health plans to cover these services and eliminating cost-sharing. In particular, services such as smoking cessation, weight loss, healthful eating, and alcohol abuse are required among new healthcare plans (US DHHS, n.d.). The Affordable Care Act provides tax incentives for worksite wellness programming and grant funding. These financial incentives could support Extension programming and research relative to worksite wellness, while addressing the most prevalent chronic diseases (overweight, obesity, CVD, hypertension) today. Ultimately, Extension has the unique opportunity to provide timely programming contributing to the research base of evidence-based practice.
References
Abood, D., Black, D., & Feral, D. (2003). Nutrition education worksite intervention for university staff: Application of the health belief model. Journal of Nutrition Education and Behavior,35:260-267. doi:10.1016/S1499-4046(06)60057-2.
Aldana, S. (2001). Financial impact of health promotion programs: a comprehensive review of the literature. American Journal of Health Promotion, 15:296-320.
American Heart Association. (2009). Heart disease and stroke statistics—2009 update. Dallas, TX: American Heart Association.
Bazzano, L. A., He, J., Ogden, L. G., Loria, C., Vupputuri, S., Myers, L., Whelton, P. K., & Johnston, S. C. (2001). Dietary potassium intake and risk of stroke in US men and women: National Health and Nutrition Examination Survey I epidemiologic follow-up study editorial comment: National Health and Nutrition Examination Survey I epidemiologic follow-up study potassium, stroke, and the bounds of epidemiological studies: National Health and Nutrition Examination Survey I epidemiologic follow-up study. Stroke. 32:1473-1480.
Berry, L. L., Mirabito, A. M. & Baun, W. B. (2010). What's the hard return on Employee Wellness Porgrams? Harvard Business Review. Retrieved from: http://hbr.org/2010/12/whats-the-hard-return-on-employee-wellness-programs/ar/1.
Blase, S. P. (1992). Worksite programming. Journal of Extension [On-line], 30(4) Article 4IAW5. Available at: https://www.joe.org/joe/1992winter/iw5.php
Block, G., Gillespie, C., Rosenbaum, E., & Jenson, C. (2000). A rapid food screener to assess fat and fruit and vegetable intake. American Journal of Preventive Medicine, 18:284-288.
Brown, J. L. & Olson, D. (1988). Taking Extension to work. Journal of Extension [On-line], 26(2) Article 2IAW3. Available at: https://www.joe.org/joe/1988summer/iw3.php
Case, P. (2010). Worksite wellness: Investing in healthy employees and economies. Journal of Extension [On-line], 48(5) Article 5FEA8. Available at: https://www.joe.org/joe/2010october/a8.php
Centers for Disease Control and Prevention. (2010). Leisure-time physical activity. Retrieved from: http://www.cdc.gov/nchs/data/nhis/earlyrelease/201003_07.pdf
Centers for Disease Control and Prevention. (2007). Eliminate disparities in cardiovascular disease. Retrieved from: http://www.cdc.gov/omhd/AMH/factsheets/cardio.htm#2
Centers for Disease Control and Prevention, Behavioral Risk Factor Surveillance System. (2007). Prevalence and trends data: Nationwide physical activity. Retrieved from: http://apps.nccd.cdc.gov/brfss/display.asp?yr=2007&cat=PA&qkey=4418&state=UB .
Chapman, L. (2003). Meta-Evaluation of Worsite Health Promotion Economic Return Studies. The Art of Health Promotion, 6:1-16.
Griffin-Blake, C. S., & DeJoy, D. M. (2006). Evaluation of social-cognitive versus stage-matched, self-help physical activity interventions at the workplace. American Journal of Health Promotion, 20:200-209.
Guenther, P., Dodd, K., Reedy, J., & Krebs-Smith, S. (2006). Most Americans eat much less than recommended amounts of fruits and vegetables. Journal of the American Dietetic Association, 106:1371-1379. doi: 10.1016/j.jada.2006.06.002.
Hunt, A., Hilgenkamp, K., & Farley, R.(2000). Skills and competencies of dietitians practicing in wellness settings. Journal of the American Dietetic Association, 100:1537-1539.
Jones, D., Peterson, E., Bonow, R., Gibbons, R. J., Franklin, B. A., Sacco, R. L., Faxon, D. P., Bufalino, V. J., Redberg, R. F., Metzler, N. M., Solis, P., Girgus, M., Rogers, K., Wayte, P., & Gardner, T. J. (2009). Partnering to reduce risks and improve cardiovascular outcomes: American Heart Association initiatives in action for consumers and patients. Circulation, 119:340-350. doi:10.1161/CIRCULATIONAHA.108.191328.
King, D., Mainous, A., Carnemolla, M., & Everett, C. (2009). Adherence to healthy lifestyle habits in US adults, 1988-2006. American Journal of Medicine, 122:528-534. doi:10.1016/j.amjmed.2008.11.013.
Kroeze, W., Oenema, A., Campbell, M., & Brug, J. (2008). Comparison of use and appreciation of a print-delivered versus CD-ROM-delivered, computer-tailored intervention targeting saturated fat intake: randomized controlled trial. Journal of Medical Internet Research, 10:e12. doi:10.2196/jmir.940.
Kroeze, W., Oenema, A., Campbell, M., & Brug, J. (2008a). The efficacy of Web-based and print-delivered computer-tailored interventions to reduce fat intake: results of a randomized, controlled trial. Journal of Nutrition Education and Behavior, 40:226-236. doi:10.1016/j.jneb.2007.09.008.
Litchfield, R. E., Muldoon, J., Welk, G., Hallihan, J., & Lane, T. (2005). Lighten up Iowa: An interdisciplinary, collaborative health promotion campaign. Journal of Extension [On-line], 43(2) Article 2FEA6. Available at: https://www.joe.org/joe/2005april/a6.php
Ludwig, D. S., Pereira, M. A., Kroenke, C. H., Hilner, J. E., Van Horn, L., Slattery, M. L., & Jacobs., D. R. (1999). Dietary fiber, weight gain, and cardiovascular disease risk factors in young adults. Journal of the American Medical Association, 282:1539-1546.
Marshall, A.L., Leslie, E.R., Bauman, A.E., Marcus, B.H., & Owen, N. (2003). Print versus website physical activity programs: A randomized trial. American Journal of Preventive Medicine, 25:88-94. doi:10.1016/S0749-3797(03)00111-9.
Mills, P., Kessler, R., Cooper, J., & Sullivan, S. (2007). Impact of a health promotion program on employee health risks and work productivity. American Journal of Health Promotion, 22:45-53.
National Health Interview Survey. (2007). Questionnaire, datasets, and related documentation 1997-present. Retrieved from: ftp://ftp.cdc.gov/pub/Health_Statistics/NCHS/Survey_Questionnaires/NHIS/2007/English/qadult.pdf
Partnership for Prevention. (2005). Leading by example: Improving the bottom line through a high performance, less costly workforce. Retrieved from: http://www.welcoa.org/pdf/LBE_Book_small.pdf
Sorensen, G., Stoddard, A., Hunt, M. K., Hebert, J. R., Ockene, J. K., Avrunin, J. S., Himmelstein, J., & Hammond, S. K. (1998). The effects of a health promotion-health protection intervention on behavior change: the WellWorks study. American Journal of Public Health, 88:1685-1690. doi:10.2105/AJPH.88.11.1685.
Sternfeld, B., Block, C., Quesenberry, C. P., Block, T. J., Husson, G., Norris, J. C., Nelson, M., & Block, G. (2009). Improving diet and physical activity with ALIVE: A worksite randomized trial. American Journal of Preventive Medicine, 36:475-483. doi:10.1016/j.amepre.2009.01.036.
Task Force Community Preventive Services. (2007). Proceedings of the task force meeting: Worksite reviews. Retrieved from: http://www.thecommunityguide.org/about/index.html
US Census Bureau. (2008). State and county quick facts. Retrieved from: http://quickfacts.census.gov/qfd/states/19000.html
US Department of Health and Human Services. (2008). Physical activity guidelines for Americans. Retrieved from: http://www.health.gov/PAGuidelines/guidelines/summary.aspx
US Department of Health and Human Services. (2006). Your guide to lowering your blood pressure with DASH. Bethesda, MD: National Institutes of Health.
US Department of Health and Human Services. (2000). Healthy people 2010: With understanding and improving health and objectives for improving health. Washington, DC: U.S. Department of Health and Human Services.
US Department of Health and Human Services. (n.d.). Understanding the Affordable Health Care Act. Retrieved from: http://www.healthcare.gov/law/introduction/index.html
US Department of Health and Human Services, US Department of Agriculture. (2005). Dietary guidelines for Americans 2005. (6th ed.) Washington, DC: U.S. Government Printing Office.