December 2020
|
December 2020 // Volume 58 // Number 6 // Feature // v58-6a5



Opportunities for Impact: Health Promotion in Rural Early Care and Education Environments
Abstract
Early care and education settings are essential partners in the battle against childhood obesity. We describe an Extension-facilitated early childhood obesity prevention intervention conducted in 25 rural early care and education settings. A total of 148 policy, systems, or environmental changes were achieved, reaching approximately 450 young children. Systems changes were the most prevalent outcome achieved. The experiences of Extension professionals in promoting policy, systems, and environmental changes are highlighted as are implications for other Extension systems and professionals promoting policy, systems, or environmental changes in early care and education settings.
Background
The prevalence of obesity among children between 2 and 5 years old in the United States doubled in recent decades (Fryar et al., 2018) and is associated with numerous negative physical and mental health consequences (Centers for Disease Control and Prevention, 2020). The National Center for Health Statistics has reported that 13.9% of children between 2 and 5 years old are classified as obese (Hales et al., 2017). Overweight and obese preschool-aged children are much more likely than their normal-weight peers to become overweight or obese adolescents and adults; therefore, the prevention of obesity in early childhood is essential to improve these alarming trends for future generations (Singh et al., 2008).
Early care and education settings (ECEs) are critical for obesity prevention, given that nearly 60% of U.S. children under 6 and not already enrolled in kindergarten attend an ECE at least part time (Center for Education Statistics, 2019). ECE providers are uniquely poised to educate children as well as parents about healthful eating and physical activity (Institute of Medicine, 2012; Story et al., 2006). Additionally, ECE providers have great potential for shaping the physical activity and nutrition behaviors of young children. Through implementation of policy, systems, and environmental (PSE) changes in ECEs, young children can benefit from increased opportunities for healthful food access and physical activity. Although ECEs are identified as important environments for promoting healthful weight in children, processes for implementing PSE changes vary widely and are often lacking, especially in rural underserved communities (Maternal and Child Health Bureau, 2015).
Cooperative Extension is a national network of educators with the knowledge and expertise to help address important health issues such as childhood obesity, yet it is underutilized for this role. Since its inception in 1914, Extension has exemplified strong collaborations across federal, state, and county governments; land-grant universities; experts; and community-based educators. Extension's initial purpose was to educate farmers on agricultural best-practices (Rogers, 1995). As the United States evolved from an agrarian society, Extension gradually expanded its focus to include the promotion of nutrition and healthful living and community-based solutions to health issues. Examples include public and private initiatives, such as Michelle Obama's Let's Move!, the Robert Wood Johnson Foundation's Building a Culture of Health, and the American Heart Association's Alliance for a Healthier Generation.
A major funding source for Extension initiatives is federal legislation called the Farm Bill, which recently added the promotion of physical activity to its nutrition education legislation (Agricultural Act, 2014). That same year, the 100th anniversary of the creation of the Extension system, the landmark Cooperative Extension Framework for Health and Wellness was published (Braun et al., 2014). The World Health Organization (WHO) has described health promotion as "a wide range of social and environmental interventions that are designed to benefit and protect individual people's health and quality of life by addressing and preventing the root causes of ill health" (WHO, 2016, para. 1). Built on the WHO's definition of health promotion and based on the socioecological model, Extension's National Framework for Health and Wellness depicts the synergistic interplay among individual, community, and societal factors. Extension is ideally suited to apply this framework to early childhood obesity prevention.
Using the multilayer approach of the framework, our team of university-level faculty in Extension and public health and county Extension staff designed the West Virginia Healthy Children Project (Bowen et al., 2020). A cooperative agreement with the Centers for Disease Control and Prevention enabled us to apply lessons learned from other state ECE efforts to the variety of ECE providers participating in our project, including Head Start, prekindergarten (pre-K) program providers, childcare centers, and family childcare homes.
We developed a hybrid intervention using the Nutrition and Physical Activity Self-Assessment for Child Care (Go NAP SACC) and I Am Moving, I Am Learning (IMIL). Both initiatives are featured in the U.S. Department of Agriculture's Supplemental Nutrition Assistance Program Education tool kit (Go NAPSACC, https://snapedtoolkit.org/interventions/programs/go-napsacc/; IMIL, https://snapedtoolkit.org/interventions/programs/i-am-moving-i-am-learning-imil/).
Go NAP SACC is designed to improve (a) the quality and quantity of healthful foods and opportunities for physical activity provided to children, (b) provider-child interactions, and (c) the potential for PSE changes related to healthful eating and physical activity. It is an updated version of the evidence-based NAP SACC program, use of which has demonstrated significant improvements in the nutrition and physical activity environments of childcare centers (Benjamin et al., 2007; Ward et al., 2008). The updates ensured that the materials were based on the most recent policies, recommendations, and scientific literature (Ward et al., 2017).
IMIL, originally developed for Head Start programs, includes resources and curriculum enhancements for integrating nutrition and physical activity into daily routines. IMIL is easy to use and has a positive impact on children and families (Allar et al., 2017; Fox et al., 2010). The signature features of IMIL are a health hero named CHOOSY (Choose Healthy Options Often and Start Young) and music embedded with health messages.
Working with ECEs is not new to Extension. In Oregon, efforts with family childcare providers revealed needed improvements in nutrition and physical activity policies and practices (Gunter et al., 2012). A preschool nutrition education program offered by Extension increased knowledge of fruits and vegetables among participating children (Niemeier et al., 2010). Cirignano (2013) exposed Extension educators to a number of resources to enhance their work in ECEs. However, ECEs were a new setting for our county Extension staff. In our project, we explored the feasibility and effectiveness of using local Extension staff to implement a hybrid of Go NAP SACC and IMIL and sought to determine whether delivering this hybrid intervention through existing Extension infrastructure would improve PSE factors related to nutrition and physical activity in ECEs.
Methods
Our project was approved by the West Virginia University Institutional Review Board. We recruited ECEs (Head Start, pre-K program providers, childcare centers, and family childcare homes) in the project's three rural counties to participate through phone calls and mailed materials. All Head Start and pre-K programs (n = 11/11), most childcare centers (n = 3/4), and approximately one third of family childcare homes (n = 11/33) elected to participate.
Prior to any interventions being introduced to ECE providers, the local Extension staff on our team who worked in the three counties participated in a Go NAP SACC online training in order to provide technical assistance to ECE providers. The local Extension staff members also were educated about the policy landscape for each ECE type in our state (e.g., national and state policies governing ECEs) and the blending of some policies when more than one ECE type operated at the same location (e.g., pre-K programs and Head Start).
We conducted training on the hybrid Go NAP SACC/IMIL intervention for ECE personnel (n = 56) from the 25 participating sites, including classroom teachers and aides, childcare center directors and staff, and family childcare owners and staff. We oriented providers to the Go NAP SACC tool, which includes guidance about how to conduct the self-assessment and set goals, and distributed copies of four self-assessment modules: Nutrition, Physical Activity, Outdoor Play and Learning, and Screen Time. Although there are slightly different versions of the self-assessments, with different numbers of items, based on ECE type, all response options comprise a 4-point Likert scale, with the fourth option always indicating alignment with best practices. The school/childcare center version contains 99 items: 45 nutrition, 22 physical activity, 20 outdoor play and learning, and 12 screen time. The family childcare version contains 91 items: 44 nutrition, 20 physical activity, 15 outdoor play and learning, and 12 screen time. Despite the availability of online self-assessments, we used printed versions due to lack of reliable internet access in the participating counties.
ECE providers completed the self-assessment modules independently. Personnel in each ECE determined how and with whom they completed the self-assessments. For example, each participating classroom teacher and aide in pre-K and Head Start programs completed the assessment together, so in those settings, the self-assessment occurred at the classroom level. In childcare centers and family childcare homes, the director/owner and relevant staff (e.g., teachers and cooks) completed the assessment, so in those settings, the process occurred at the facility level.
The trained local Extension staff members met with providers to set goals based on their self-assessments and discuss possible solutions for moving toward best practices. In addition to providing technical assistance, the local Extension staff tracked ECE goals and progress over the course of the project. Each ECE provider identified barriers, and the Extension staff helped minimize or remove the barriers to encourage and enable best practices. We provided resources to ECE providers to help them accomplish their goals and to reinforce key messages of healthful eating and physical activity. Examples of the resources are as follows:
- materials featuring CHOOSY to promote healthful eating and movement;
- CHOOSY visits during which children engaged in physical activity through song and dance;
- CHOOSY-inspired messages and music CDs to send home;
- seasonal produce for families coordinated by agricultural Extension staff and local farmers;
- resources to support garden-based learning, such as raised beds, gardening tools, soils, seeds, and children's literature; and
- portable play equipment (e.g., tricycles and balls) and cooking resources (e.g., grill pans).
Overall, the local Extension staff provided ECE providers with the guidance and resources needed to accomplish their goals.
Analysis
Self-Assessment
We entered responses from providers' self-assessments into a database for analysis and coded responses "1" if the ECE met best practice and "0" if it did not. Frequency of best practice was calculated for each item by ECE type (school/center and family childcare) and module topic (nutrition, physical activity, outdoor play and learning, and screen time). Responses were deemed a strength if greater than 50% of the ECEs reported best practice and an opportunity for improvement if less than 50% of the ECEs reported best practice.
Goal Status
We tracked the number of goals set and the status of each goal over a 2-year period by categorizing goals as met/ongoing, partially met, or not met and then classifying goals met/ongoing as policy (P), systems (S), or environmental (E) changes using established definitions (The Food Trust, 2012):
- policy—written statement of organizational position, decision, or course of action;
- systems—unwritten, ongoing organizational decisions or changes that result in new activities; and
- environmental—physical, observable changes in the built, economic, and/or social environment.
Two members of our team independently classified the goals into P, S, or E categories and resolved discrepancies by consensus.
Results
Self-Assessment
Tables 1–4 display selected data (percentages of ECEs meeting best practices) categorized as strengths and opportunities for improvement for pre-K, Head Start and childcare centers for each module.
| Best practice by category |
ECEs meeting best practice % |
|---|---|
| Strengths | |
| Children are not often given sweet or salty snacks outside of mealtime. | 100 |
| High-sugar, high-fat foods are offered less than one time a week or never. | 89 |
| Fried or prefried meats or fish offered less than one time a week or never. | 82 |
| TVs or videos are never on during meal/snack times. | 100 |
| Children rarely or never are required to sit at table until they clean their plate. | 100 |
| Food is rarely or never used to calm upset children or encourage appropriate behavior. | 94 |
| Opportunities | |
| Families are offered education on child nutrition two times a year or more. | 29 |
| Flavored milk is never offered. | 13 |
| High-fiber, whole-grain foods offered two times a day or more. | 28 |
| 4- to 6-oz serving of 100% fruit juice is offered two times a week or less. | 24 |
| A large variety of posters, books, and other learning materials that promote healthful eating are available. | 28 |
| Written policy on child nutrition includes nine or 10 specified topics. | 25 |
| Note. ECE = early care and education setting. | |
| Best practice by category |
ECEs meeting best practice % |
|---|---|
| Strengths | |
| Indoor play space includes three or four specified features. | 72 |
| Outside of meal/snack times, the longest children are asked to remain seated at any one time is less than 15 min. | 63 |
| Teachers/providers never take away physical activity or remove child from physically active playtime to manage challenging behaviors for longer than 5 min. | 69 |
| Teachers/providers supervise, verbally encourage, and often join in to increase children's physical activity. | 75 |
| Planned lessons on gross motor skills are offered one time a week or more. | 88 |
| Opportunities | |
| 60 min or more a day of adult-led physical activity is provided. | 6 |
| Families are offered education on child physical activity two times a year or more. | 17 |
| Professional development on child physical activity is completed two times a year or more. | 18 |
| A large variety of posters, books, and other learning materials that promote physical activity are available. | 22 |
| Written policy on physical activity includes seven or eight specified topics. | 28 |
| Note. ECE = early care and education setting. | |
| Best practice by category |
ECEs meeting best practice % |
|---|---|
| Strengths | |
| The outdoors is used for four or five specified activity types. | 75 |
| One half to three quarters of outdoor play space is shaded by structures or trees. | 100 |
| Gardens grow enough fruits/vegetables to provide children meals or snacks during one or more seasons. | 100 |
| Open area used for outdoor games, activities, and events is large enough for most children to run around safely. | 82 |
| Opportunities | |
| Outdoor playtime is provided three times a day or more. | 0 |
| Families are offered education on outdoor play and learning two times a year or more. | 22 |
| Professional development on outdoor play and learning is competed two times a year or more. | 24 |
| Written policy on outdoor play and learning includes six or seven specific topics. | 22 |
| Note. ECE = early care and education setting. | |
| Best practice by category |
ECEs meeting best practice % |
|---|---|
| Strengths | |
| Less than 30 min or no screen time is allowed for children 2 years and older. | 87 |
| When screen time is offered, teachers always talk with children about what they are seeing/learning. | 71 |
| Screen time is rarely or never used as a reward. | 82 |
| Opportunities | |
| Professional development on screen time is completed two times a year or more. | 11 |
| Families are offered education on screen time two times a year or more. | 22 |
| Written policies about screen time include five or six specific topics. | 28 |
| Note. ECE = early care and education setting. | |
Tables 5–8 display selected data (percentages of ECEs meeting best practices) categorized as strengths and opportunities for improvement for family childcare homes for each module.
| Best practice by category |
ECEs meeting best practice % |
|---|---|
| Strengths | |
| Fresh, frozen canned (juice) fruit is offered every time fruit is served. | 100 |
| High-salt, high-fat snacks are offered less than one time a week or never. | 82 |
| High-sugar, high-fat foods are offered less than one time a week or never. | 74 |
| Fried or prefried potatoes are offered less than one time a week or never. | 89 |
| TVs or videos are never on during meal/snack times. | 100 |
| Children are rarely or never required to sit at table until they clean their plate. | 91 |
| Opportunities | |
| High-fiber, whole-grain foods are offered two times a day or more. | 37 |
| 4- to 6-oz serving of 100% fruit juice is offered two times a week or less. | 27 |
| Fat-free milk is offered for children 2 years and older. | 11 |
| Families are offered education on child nutrition two times a year or more. | 33 |
| A large variety of posters, books, and other learning materials that promote healthful eating are available. | 0 |
| Written policy on child nutrition includes six to nine specified topics. | 18 |
| Note. ECE = early care and education setting. | |
| Best practice by category |
ECEs meeting best practice % |
|---|---|
| Strengths | |
| 45 min or more a day of adult-led physical activity is provided. | 78 |
| Outside of meal/snack times, the longest children are asked to remain seated at any one time is less than 15 min. | 90 |
| Providers never take away physical activity or remove child from physically active playtime to manage challenging behaviors for longer than 5 min. | 73 |
| Provider supervises, verbally encourages, and often joins in to increase children's physical activity. | 73 |
| Opportunities | |
| Families are offered education on child physical activity two times a year or more. | 17 |
| Professional development on child physical activity is completed two times a year or more. | 18 |
| A large variety of posters, books, and other learning materials that promote physical activity are available. | 22 |
| Written policy on physical activity includes seven or eight specified topics. | 28 |
| Note. ECE = early care and education setting. | |
| Best practice by category |
ECEs meeting best practice % |
|---|---|
| Strengths | |
| The outdoors is used for four specified activity types. | 78 |
| Open area used for outdoor games, activities, and events is large enough for most children to run around safely. | 82 |
| Children are always offered portable play equipment during outdoor playtime. | 73 |
| Opportunities | |
| One half to three quarters of outdoor play space is shaded by structures or trees. | 38 |
| Families are offered education on outdoor play and learning two times a year or more. | 11 |
| Written policy on outdoor play and learning includes six or seven specific topics. | 0 |
| Note. ECE = early care and education setting. | |
| Best practice by category |
ECEs meeting best practice % |
|---|---|
| Strengths | |
| When screen time is offered, teachers always talk with children about what they are seeing/learning. | 67 |
| Screen time is rarely or never used as a reward. | 67 |
| Opportunities | |
| No TVs are present or TVs are kept out of rooms where children spend most of the day. | 11 |
| Professional development on screen time is completed two times a year or more. | 11 |
| Families are offered education on screen time two times a year or more. | 0 |
| Written policies about screen time include five or six specific topics. | 10 |
| Note. ECE = early care and education setting. | |
Goal Status
Participants set a total of 185 goals across ECE types: pre-K and Head Start classroom teachers, 102 goals (average of nine goals per classroom); childcare center directors/staff, 13 goals (average of four goals per site); and family childcare owners/staff, 69 goals (average of six goals per site). Figure 1 displays the percentages of goals set by category, and Figure 2 displays the percentages of goals reported as met by category.
Figure 1.
Goals Set by Category
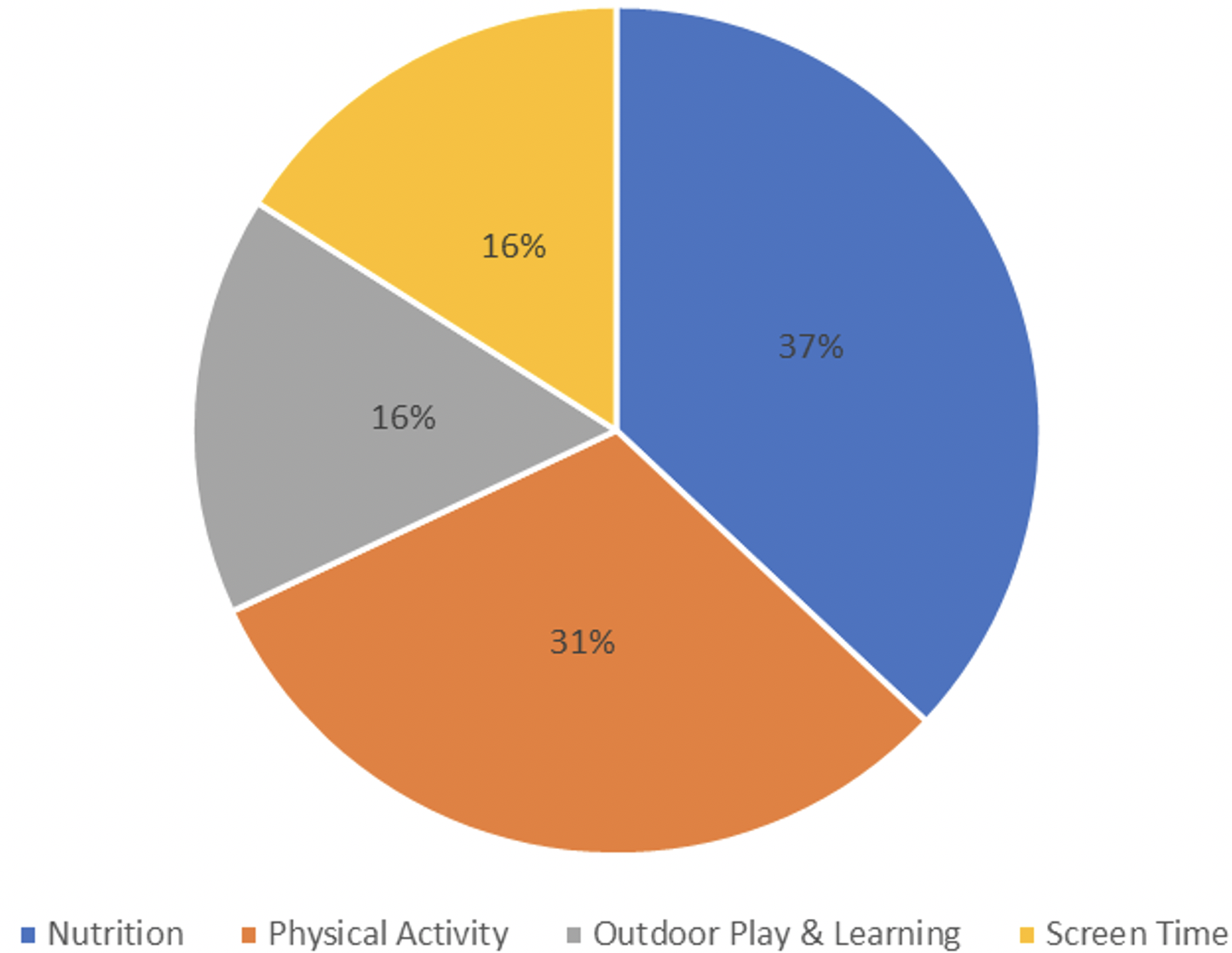
Figure 2.
Goals Reported as Met by Category
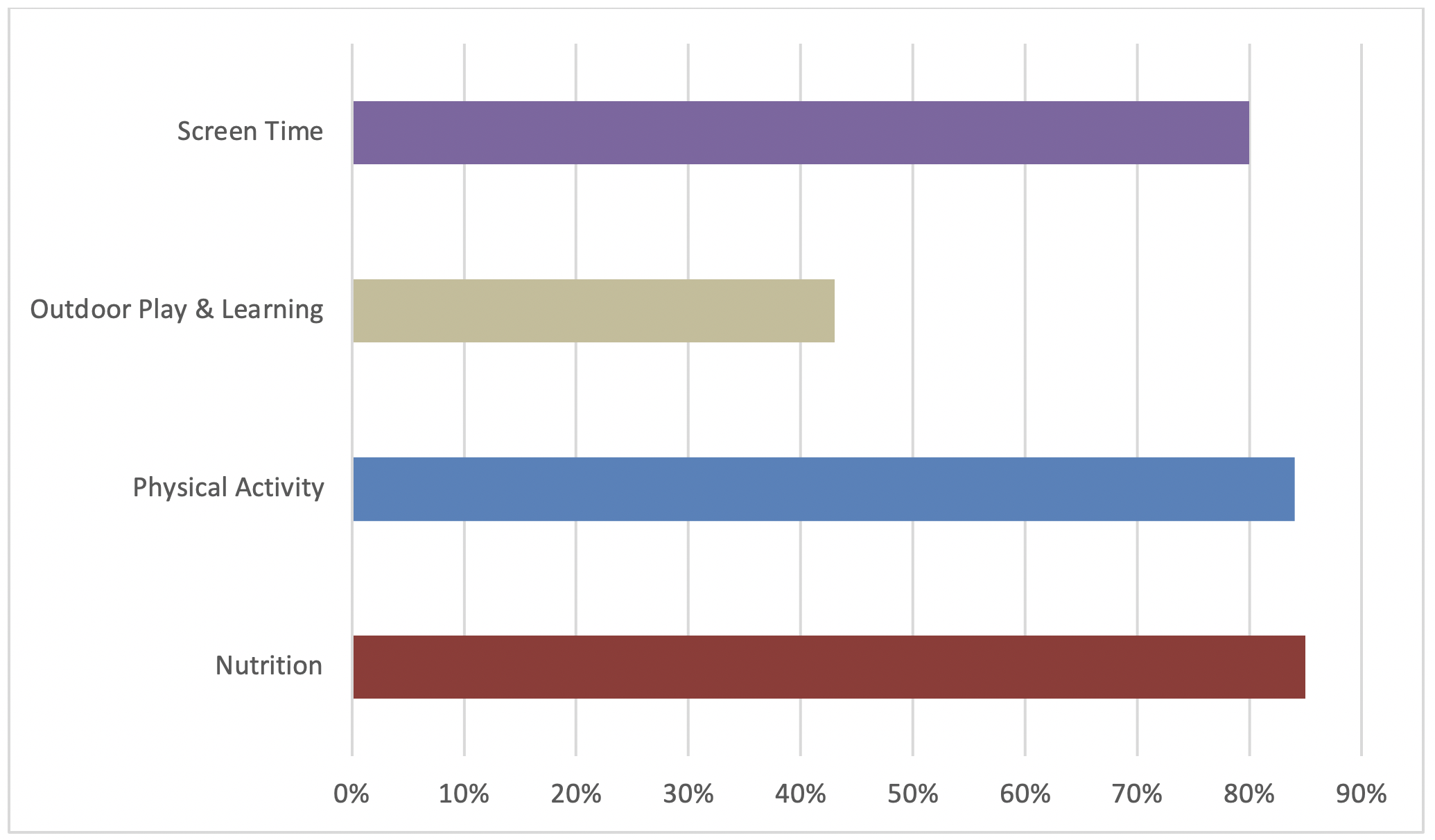
The higher percentages of nutrition and physical activity goals set and met are likely attributable to the higher numbers of items in those modules; providers literally had more options to choose from. The lower percentages of outdoor play and learning goals set and met occurred primarily among the family childcare providers, who expressed having more limited opportunities to provide shade in outdoor play spaces and time/capacity for education for families and professional development.
The interactions between the local Extension staff and ECE providers were largely positive. Table 9 displays examples of best practice and goal setting issues discussed by members of the two groups and the outcomes of those interactions. Most often, the interactions occurred between Extension staff and ECE providers, but in some cases, Extension staff interacted with other ECE key personnel. For example, in one case a pre-K classroom teacher referred the Extension staff member to the school food service director to discuss moving to the best practice of not serving flavored milk. This interaction required the Extension staff member to be knowledgeable about state nutrition policies in addition to Go NAP SACC best practices.
| Topic | ECE type | Issue discussed | Outcome/resolution |
|---|---|---|---|
| Nutrition | Pre-K | Water was not allowed in the classroom. | Water bottles are allowed in the classroom. |
| Pre-K | Two types of flavored milk (1%) were offered. | Flavored milk is limited to one type. | |
| Childcare center | Staff did not eat meals with children. | Staff eats with children. | |
| Head Start | Children who requested more food were not asked whether they were still hungry before they were served more food. | Teachers ask children whether they are still hungry before serving them more food. | |
| Physical activity | Pre-K | Physical activity equipment was not available during free play. | Physical activity equipment is available during free play. |
| FCC | Limited opportunities for gross motor skill development existed. | Gross motor skills are incorporated one or more times a week. | |
| FCC | Adult-led physical activity was lacking. | 30 min of adult-led physical activity is provided on most days. | |
| Outdoor play and learning | Childcare center | Equipment for outdoor play was lacking. | Outdoor play equipment was obtained. |
| Screen time | Pre-K | Parent education on screen time was lacking. | Teacher conducted a parent training about limiting screen time. |
| FCC | Noneducational and commercial (advertising) screen time was allowed. | Screen time is limited to commercial-free/educational programming. | |
| Note. FCC = family childcare homes. | |||
Table 10 shows the results of our content analysis of classifying goals met as P, S, or E changes. Four percent of all goals met were policy related. Examples of adopted policies included requiring that teachers sit with children during mealtimes and consume the same foods, that 120 min of daily physical activity be provided, and that screen time be limited to commercial-free and educational programs. Sixty-eight percent of goals met were system/practice changes. Examples of such changes included providing more adult-led physical activity; increasing time for outdoor play; and providing more nutrition, physical activity, and screen time education to parents. Twenty-eight percent of goals met were environmental changes. These related to making water readily available, increasing offerings of fruits/vegetables and dark vegetables, providing more portable play equipment, and enhancing outdoor play space. Specific examples include the addition of container gardens (outdoors and in classrooms), outdoor water fountains, and shaded environments for outdoor play. Approximately 450 children were reached by these changes.
| Topic area | Policy change | Systems change | Environmental change | Total PSE goals |
|---|---|---|---|---|
| Nutrition | 2 | 34 | 22 | 58 |
| Physical activity | 3 | 36 | 8 | 47 |
| Outdoor play and learning | 0 | 10 | 9 | 19 |
| Screen time | 1 | 21 | 2 | 24 |
| Total | 6 (4%) | 101 (68%) | 41 (28%) | 148 |
We framed each provider's policies to display publicly. Figure 3 shows an example of such a display—policy language developed by a pre-K classroom teacher with CHOOSY in the background.
Figure 3.
Sample Policy Language
Discussion and Implications for Extension
ECE recruitment was successful, with the exception of recruitment of family childcare homes. Although we made multiple contacts by telephone, email, and postal mail, some providers never responded. Ward et al. (2016) characterized family childcare providers as having unique challenges as compared to other ECE providers, including little or no staff support and greater time constraints. Further, these providers may be reluctant to participate in initiatives that seem related to licensure or monitoring. We framed our project as not being associated with licensing and emphasized that it would complement and enhance what they already do. Our experience is that family childcare providers were much harder to reach than the other ECE providers, perhaps because they were not part of a formal system such as a school. Future efforts with family childcare homes should include planning for the unique challenges associated with this type of ECE and developing enhanced recruitment plans.
We are not surprised that policy was the least prevalent kind of change achieved. Some of the Go NAP SACC policies were out of the purview of certain types of providers. For example, it was difficult for us to move the needle on flavored milk in pre-Ks operating in public schools because existing state policy allows flavored milk in public schools. Conversely, screen time was not an issue for pre-K classrooms because of a strong state policy. However, addressing screen time was challenging with family childcare providers, many of whom were unwilling to move televisions out of child play areas or reduce the amount of time televisions were turned on. This circumstance is consistent with other research on family childcare homes, which has shown that televisions often are on for at least part of every day (Trost et al., 2009). We also struggled with helping these providers create site-specific policies, a challenge that other researchers have encountered (Francis et al., 2018). However, several providers did incorporate nutrition-related policy language into their handbooks, including language related to not offering flavored milk or fruit juice. Providers also enhanced their healthful eating message environment by increasing the availability of books, posters, and other learning materials that promote healthful eating.
Also, as expected, systems changes were the most prevalent changes achieved. These types of actions may be more attainable as most are in the purview of ECE providers. Importantly, our philosophy was to respect the context in which providers operate and not be critical. Instead of focusing on the deficits identified in their self-assessments, our Extension staff emphasized learning about best practices and making positive changes toward best practices. Through the self-assessment process, ECE providers gained a better understanding of how their policies and practices compared with best practices. We believe this approach helped raise providers' awareness of their health-promoting role and are optimistic that they will continue to move toward best practices.
IMIL was quite instrumental in enabling providers to increase the amount of adult-led daily physical activity. The ready-to-use songs and dances were accessible and easy to use, with little preparation or planning required. These characteristics are identified as critical (Glasgow & Emmons, 2007) and illustrate the synergy between Go NAP SACC and IMIL: Go NAP SACC identified best practices, and IMIL provided a creative means for achieving them.
According to Walsh et al. (2018), "moving from working on behavior change through direct education to working to change the behavioral context and systems . . . [is] a deep shift that would require developing a system-wide shared vision and value for this new way of working" for Extension (p. 45). Although working with ECEs to promote PSE changes was relatively new to local Extension staff in our project, they enhanced their PSE-related literacy and gained skills in motivational interviewing and mentoring, which can be applied to other initiatives.
Our project involved Extension staff with expertise in family life, youth development, community development, and agriculture. We intentionally connected to gardening and learning about food production, and this aspect of the project was very well received by ECE providers. When Extension collaborates internally across program areas, as in our project, there are significant benefits to the organization, its employees, and communities served.
A limitation of our project is that we were not able to track its long-term impact on child overweight or obesity. However, given the national adult prevalence rates of obesity (42%) and severe obesity (11%) forecasted through 2030, a focus on early primary prevention is imperative (Finkelstein et al., 2012). Continued efforts are needed to implement interventions in ECEs as well as to understand the contexts within which young children and their caregivers live (Haire-Joshu & Tabak, 2016). The experiences of our team highlight the need for Extension to seize opportunities for health promotion within ECEs.
Author Note
The research reported in this publication was supported by Cooperative Agreement Number 5NU58DP005488-02-00 from the Centers for Disease Control and Prevention. Its contents are solely the responsibility of the authors and do not necessarily represent the official view of the Centers for Disease Control and Prevention.
We wish to thank the dedicated ECE professionals in our project who strive to provide nurturing and healthful environments for young children.
Correspondence concerning this article should be addressed to Nancy O'Hara-Tompkins. Email: ntompkins@hsc.wvu.edu
References
Agricultural Act of 2014, Pub. L. No. 113-79 (2014). https://www.agriculture.senate.gov/imo/media/doc/Agricultural%20Act%20of%202014.pdf
Allar, I., Jones, E., Elliott, E., Kristjansson, A., Taliaferro, A., Mann, M., & Bulger, S. (2017). The perceived impact of I am Moving, I am Learning on physical activity and family involvement: A preliminary investigation. American Journal of Health Behavior, 41(6), 683–692. https://doi.org/10.5993/AJHB.41.6.2
Benjamin, S. E., Ammerman, A., Sommers, J., Dodds, J., Neelon, B., & Ward, D. S. (2007). Nutrition and physical activity self-assessment for childcare (NAP SACC): Results from a pilot intervention. Journal of Nutrition Education & Behavior, 39(3), 142–149. https://doi.org/10.1016/j.jneb.2006.08.027
Bowen, E., Murphy, E., O'Hara-Tompkins, N., Crum, G., Fincham, H., & Burkhart-Polk, M. (2020). Early childhood obesity prevention in rural West Virginia: Extension's role and lessons learned. Journal of Human Sciences, 8(1), 163–177.
Braun, B., Bruns, K., Cronk, L., Kirk Fox, L., Koukel, S., Le Menestrel, S., Lord, L. M., Reeves, C., Rennekamp, R., Rice, C., Rodgers, M., Samuel, J., Vail, A., & Warren, T. (2014). Cooperative Extension's framework for health and wellness. https://nifa.usda.gov/resource/national-framework-health-and-wellness
Center for Education Statistics. (2019). Early childhood program participation, results from the National Household Education Surveys Program of 2016. U.S. Department of Education. https://nces.ed.gov/pubs2017/2017101REV.pdf
Centers for Disease Control and Prevention. (2020, September 2). Childhood obesity causes & consequences. https://www.cdc.gov/obesity/childhood/causes.html
Cirignano, S. M. (2013). Using current resources to implement wellness programming for preschoolers. Journal of Extension, 51(5), Article v51-5tt9. https://joe.org/joe/2013october/pdf/JOE_v51_5tt9.pdf
Finkelstein, E., Khavjou, O., Thompson, H., Trogdon, J. G., Pan, L., Sherry, B., & Deitz, W. (2012). Obesity and severe obesity forecasts through 2030. American Journal of Preventive Medicine, 42(6), 563–570. https://doi.org/10.1016/j.amepre.2011.10.026
Fox, M. K., Hallgren, K., Boller, K., Turner, A., Cabili, C., Condon, E., Grosso, P., Eden, D., Finkelstein, D., Kennen, B., & Esposito, A. M. (2010). Efforts to meet children's physical activity and nutritional needs: Findings from I am Moving I am Learning implementation evaluation. U.S. Department of Health & Human Services, Administration for Children and Families. https://www.mathematica-mpr.com/-/media/publications/pdfs/earlychildhood/iml_implement_eval.pdf
Francis, L., Shodeinde, L., Black, M., & Allen, J. (2018). Examining the obesogenic attributes of the family child care home environment: A literature review. Journal of Obesity, 2018, Article 3490651. https://doi.org/10.1155/2018/3490651
Fryar, C. D., Carroll, M. D., & Ogden, C. L. (2018). Prevalence of overweight, obesity and severe obesity among children and adolescents aged 2–19 years: United States, trends 1963–1965 through 2015–2016. (Health E-Stats). Centers for Disease Control and Prevention, National Center for Health Statistics. https://www.cdc.gov/nchs/data/hestat/obesity_child_15_16/obesity_child_15_16.htm#table1
Glasgow, R. E., & Emmons, K. M. (2007). How can we increase translation of research into practice? Types of evidence needed. Annual Review of Public Health, 28, 413–433. https://doi.org/10.1146/annurev.publhealth.28.021406.144145
Gunter, K. B., Rice, K. R., & Trost, S. T. (2012). Nutrition and physical activity policies and practices in family child care homes in Oregon: Baseline findings from the Healthy Home Child Care project. Journal of Extension, 50(3), Article v50-3a3. https://joe.org/joe/2012june/a3.php
Haire-Joshu, D., & Tabak, R. (2016). Preventing obesity across generations: Evidence for early life intervention. Annual Review of Public Health, 37, 253–271. https://doi.org/10.1146/annurev-publhealth-032315-021859
Hales, C. M., Carroll, M. D., Fryar, C. D., & Ogden, C. L. (2017). Prevalence of obesity among adults and youth: United States 2015–2016. (Data Brief No. 288). Centers for Disease Control and Prevention, National Center for Health Statistics. https://www.cdc.gov/nchs/data/databriefs/db288.pdf
Institute of Medicine. (2012). Accelerating progress in obesity prevention: Solving the weight of the nation. National Academies Press.
Maternal and Child Health Bureau. (2015). The health and well-being of children in rural areas: A portrait of the nation, 2011–2012. U.S. Department of Health and Human Services, Health Resources and Services Administration. https://mchb.hrsa.gov/nsch/2011-12/rural-health/pdf/rh_2015_book.pdf
Niemeier, B. S., Tande, D. L., Hwang, J., Stastny, S., & Hektner, J. M. (2010). Using education, exposure, and environments to increase preschool children's knowledge about fruit and vegetables. Journal of Extension, 48(1), Article v48-1iw6. http://www.joe.org/joe/2010february/iw6.php
Rogers, E. M. (1995). Diffusion of innovations (4th ed.). Free Press.
Singh, A. S., Mulder, C., Twisk, J. W., Mechenlen, W., & Chinapaw, M. J. (2008). Tracking of childhood overweight into adulthood: A systematic review of the literature. Obesity Reviews, 9(5), 474–488. https://doi.org/10.1111/j.1467-789X.2008.00475.x
Story, M., Kaphingst, K. M., & French, S. (2006). The role of childcare settings in obesity prevention. Future of Children, 6(1), 143–168. https://doi.org/10.1353/foc.2006.0010
The Food Trust. (2012). What is policy, systems and environmental (PSE) change? http://healthtrust.org/wp-content/uploads/2013/11/2012-12-28-Policy_Systems_and_Environmental_Change.pdf
Trost, S. G., Messner, L., Fitzgerald, K., & Roths, B. (2009). Nutrition and physical activity policies and practices in family childcare homes. American Journal of Preventive Medicine, 37(6), 537–540. https://doi.org/10.1016/j.amepre.2009.09.020
Walsh, M., John, D., Peritore, N., Morris, A., Bird, C., Ceraso, M., Eichberger, S., Novotny, R., Stephenson, L., Stluka, S., & Riportella, R. (2018). Health in all policies: Working across sectors in Cooperative Extension to promote health for all. Journal of Human Sciences and Extension, 6(2), 37–56. https://www.jhseonline.com/article/view/718/620
Ward, D. S., Benjamin, S. E., Ammerman, A. S., Ball, S. C., Neelon, B. H., & Bangdiwala, S. I. (2008). Nutrition and physical activity in childcare: Results from an environmental intervention. American Journal of Preventive Medicine, 35(4), 352–356. https://doi.org/10.1016/j.amepre.2008.06.030
Ward, D. S., Vaughn, A. E., Burney, R. V., & Ostbye, T. (2016). Recruitment of family child care homes for an obesity prevention intervention study. Contemporary Clinical Trials Communication, 3, 131–138.
Ward, D. S., Vaughn, A. E., Mazzucca, S., & Burney, R. V. (2017). Translating a childcare based intervention for online delivery: Development and randomized pilot study of Go NAPSACC. BMC Public Health, 17, 891. https://doi.org/10.1186/s12889-017-4898-z
World Health Organization. (2016, August 20). What is health promotion? https://www.who.int/news-room/q-a-detail/what-is-health-promotion