August 2020
|
August 2020 // Volume 58 // Number 4 // Research In Brief // v58-4rb2



Addressing Facilitators and Barriers Related to Early Childhood Obesity Prevention in Rural Appalachian Communities
Abstract
Through a community-focused needs assessment conducted in rural Appalachia, we gauged perceptions of facilitators and barriers related to healthful eating and physical activity for young children and identified suggestions for improvement. Thirty-seven key informant interviews and three caregiver focus group sessions were coded and analyzed for key themes. Limited community resources emerged as a barrier to both healthful eating and physical activity. Suboptimal communication about existing opportunities was also identified. Community members reviewed the needs assessment data and implemented initiatives to address identified needs. The importance of Extension-facilitated needs assessments in rural settings to shape health initiatives to local contexts is highlighted.
Background
The prevalence of childhood obesity has nearly tripled over the past 30 years as approximately 17% of children and adolescents aged 2–19 years are obese (Centers for Disease Control and Prevention, 2018). Preventing obesity in early childhood is a public health priority because childhood obesity often leads to adult obesity and is challenging to reverse if children are obese by age 5 (Cunningham, Kramer, & Narayan, 2014). A focus on rural children is particularly warranted as they are at higher risk for developing obesity than their metropolitan counterparts (Johnson & Johnson, 2015). Numerous barriers to healthful eating and physical activity (PA) for young children in rural and low-income communities have been identified, including social norms that promote unhealthful eating (Seguin, Connor, Nelson, Lacroix, & Eldridge, 2014), long distances to relevant destinations, (Finklestein, Petersen, & Schottenfeld, 2017), and built environment challenges (e.g., limited sidewalks) (Hessler, 2009).
Herein we describe (a) a needs assessment we conducted in West Virginia prior to implementation of a childhood obesity prevention project in early care and education settings (Bowen et al., 2020) and (b) the community-wide actions taken to address identified needs. Our team comprised university faculty from Extension and Public Health as well as county-level Extension professionals. Intended audiences for this article include Extension professionals addressing early childhood obesity prevention in rural settings who aim to change not only individual behavior but also the broader environment in which young children and families live.
West Virginia, a predominantly rural state and the only state entirely in Appalachia, has high mortality rates for obesity-related diseases such as heart disease, stroke, cancer and type 2 diabetes (Appalachian Regional Commission, 2017). Our needs assessment, which was funded as part of the Centers for Disease Control and Prevention High Obesity Project (Murriel, Kahin, Pejavara, & O'Toole, 2020), coincided with two major shifts in the Extension world: the addition of PA promotion to the Farm Bill in 2014 (Harden, Gunter, & Lindsay, 2018; U.S. Department of Agriculture Farm Service Agency, 2014) and Extension's assuming a more public health–oriented approach with the adoption of Cooperative Extension's National Framework for Health and Wellness (Braun et al., 2014). These shifts were accompanied by expectations that Extension professionals would promote healthful eating and PA in the context of the social ecological model (SEM) (Sallis & Owen, 2015). The SEM is a multilevel approach that promotes policy, systems, and environmental (PSE) changes rather than focusing solely on the individual level (Leeman, Myers, Ribisl, & Ammerman, 2015; Murriel et al., 2020; Smathers & Lobb, 2015). A recent survey of Extension professionals revealed a less than thorough understanding of PSE changes (Smathers et al., 2019).
Methods
We conducted key informant interviews and caregiver focus group sessions in the three counties involved in our project. Key informant interviews and focus group session protocols and analytic procedures were similar, with slight variations in recruitment, sampling, and questions. The project was approved by the West Virginia University Institutional Review Board, and participants in both the key informant interviews and focus group sessions consented to have their responses audio-taped and findings reported in the aggregate.
The county-level Extension professionals on our team identified key informants in their communities to represent a variety of sectors, including public office, education, health, parks and recreation, youth sports organizations, and faith-based organizations. We conducted 37 key informant interviews in all.
We recruited focus group participants through communications conducted via the county Extension offices, flyers sent home from early care and education settings, local print and radio advertisements, and word of mouth. A total of 26 caregivers participated in the three focus group sessions, with 11, nine, and six participants in the respective sessions. We provided a $35 gift card incentive to each focus group participant, and childcare was available. At the beginning of each session, we asked focus group participants to complete a brief demographic questionnaire.
We developed a structured script for the key informant interviews and the focus group sessions, modified with permission from similar research (Fialkowski et al., 2014). The key informant interviews took approximately 45 min per informant, and the focus group sessions lasted between 2 and 2.5 hr. Our facilitators led each focus group session, with at least one other team member recording written notes to supplement the audio recording. Table 1 displays sample questions from both the key informant interviews and the focus group sessions.
| Study component | Sample questions |
|---|---|
| Key informant interviews |
What is your role in the community, and how long have you been in that role? How does your community promote healthy eating and physical activity for young children between 2 and 5 years of age? Who are the people or organizations in your community that promote healthy eating? What can you do or change in your community to help young children eat more healthfully? Where are healthy foods available in your community? Do restaurants and food establishments in your community offer healthy food? Are there enough options to purchase healthy food in your community? What are ways you can increase healthy food consumption in your community? Where are fruits and vegetables available in your community? What are ways or resources to increase fruit and vegetable availability in your community? What community changes or community-based approaches can you think of that help encourage young children to drink more water? What policies or programs can your community promote or enact to discourage consumption of sugar-sweetened beverages? What existing programs, policies, and other resources support young children to be physically active in your community? What do you believe could be done to improve/increase physical activity for young children in the community? What makes it easy for young children to spend time in front of a screen? If you wanted young children in your community to spend less time in front of a screen, what changes in your community or your surroundings would you recommend? Who are the people or organizations in your community who promote physical activity for young children? What are the best ways to get information on healthy eating and being active to families in your community? What can we do to make children eating healthier and being physically active a priority in the community? If changes were made in your community to increase healthy eating and physical activity for young children, how do you think residents would respond? What barriers or challenges would need to be overcome? |
| Focus group sessions |
Ice breaker: Facilitator asks participants to share three things about themselves: (1) how many children they care for, (2) favorite place to eat in their community, and (3) favorite physical activities. Are healthy eating and being physically active discussed openly in this community? If they are, where and why? Are healthy eating and being physically active talked about at home? Think about your younger children—do you talk with them about healthy eating and being physically active? What about with extended family? What changes can be made at home to get young children to eat more healthy foods and to drink more water and drink less sugar-sweetened beverages? The next question is about early care and education settings—places like child care centers, preschools, babysitters, and Head Start child care centers. Are healthy eating and physical activity talked about there? What changes can be made to those settings to promote healthy foods and to get young children to drink more water and drink fewer sugar-sweetened beverages? What do you think communities, families, schools, or others in the community can do to encourage young children to eat healthy and be physically active? What in your community might contribute to young children not eating healthy or not being physically active? Which of these could be easily changed? I want you to help really narrow this down. What does your community need? Or what would help young children eat healthier and be physically active? What's missing from your community to help? What are some of the reasons that less healthy foods are chosen over healthy foods in your community? What about any policies? Are there any policies in [community] that prevent people from eating healthy or from being physically active? Can you use the playgrounds at your schools? What programs, events, activities that happen here, in [community], help people be healthy or be physically active, and where do you find them? If the answer is "There are none," tell me that. What programs or other resources would help families support healthy eating and being physically active? What changes to the community or your surroundings would you recommend to decrease screen time and increase active play? Who or what are the healthy role models for children in your community? And I'm not asking you to name any individuals, but what their title is or what their role is. So who are the role models in this community, the healthy role models for the children? If you could identify three things that young children 2 to 5 years of age in your community need to develop healthy eating and physical activity behaviors, what are they? If you could identify three things that young children 2 to 5 years of age need in early care and education settings (preschool, child care center, in-home family care provider) to eat healthier and be more physically active, what would those be? Thinking outside the box, what are some ideas, policies, programs, or activities you can think of that can help your community and early care and education settings in your community help kids eat healthy and be active? |
Analysis
All recordings were transcribed verbatim and independently reviewed by two members of our team using a uniform codebook. The codebook was developed first using core categories based on the question guides, which represented topics of primary interest. Additional subcore categories were added to provide more detail or to provide a particular context for the core categories. The two reviewers compared their independently derived codes and resolved any coding discrepancies through consensus. One additional reviewer on our team reviewed all transcripts for consistency.
Coded transcripts were entered in Atlas Ti software (v.7.5.18) for thematic analysis. Two main categories (healthful eating and PA) and three subcategories (facilitators, barriers, and suggestions) formed the organizing framework for the thematic analysis. Themes were identified on the basis of number of coded responses and descriptive quotations. Data saturation was achieved when no new themes emerged in both the key informant interviews and focus group sessions.
Results
The 37 key informants represented the following sectors: public schools (n = 10), local government (n = 7), health/health care (n = 6), parks, recreation, and sports (n = 4), faith-based organizations (n = 4), local coalitions (n = 3), youth-serving organizations (n = 2), and a farmers' market (n = 1).
Eleven, nine, and six caregivers participated in the three focus group sessions, respectively. All identified as White/Caucasian. The average age of participants was 33 years; ages ranged from 19 to 60 years. Most participants (81%) were female, and the length of time they had resided in their counties ranged from 3 to more than 45 years (average length of residency was 21 years).
In general, eating was discussed more often than PA during the key informant interviews, whereas caregivers in the focus groups commented more about PA. Overall, barriers were mentioned more often than facilitators by both key informants and caregivers. A barrier was mentioned almost twice as often as a facilitator during key informant interviews and more than twice as often during caregiver sessions. Both key informants and caregivers offered several suggestions and ideas for their communities.
Key Informant Interview Results
Table 2 displays facilitator, barrier, and suggestion key concepts and supportive quotes from the key informant interviews for each topic area (healthful eating and PA).
| Key concept | Supporting quotes |
|---|---|
| Healthful eating facilitators | |
| Gardens, farmers' markets, and strong beverage policies support health. |
KI-5: A lot of people around here do have their own gardens. KI-6: There is a farmers' market that starts in the summer . . . It's right downtown and within walking distance of the neighborhoods. KI-7: We don't allow anything here except plain water. No colored water, no flavored water, no nothing, [and] no juices. |
| Healthful eating barriers | |
| Cost, lack of adult skills in food preparation, and availability of water are concerns. |
KI-8: Certain parents are afraid to buy them [vegetables]—because especially if they are on a fixed income, or say they only have the $10 voucher. Why would they purchase an eggplant if they don't even know if their child will even eat it? KI-9: The city park doesn't even have a water fountain in it. So, we're begging for the kid to go and buy a pop or an energy drink. That would help if we had water fountains out instead of pop machines. KI-10: I've been in food service or family service science with schools in West Virginia since 1975, and I'm just really concerned about the path that we're taking. I don't think people are entering adulthood with the skills they need to properly know what they should or should not be feeding. |
| PA facilitators | |
| Education about the negative effects of screen time and availability of PA resources are strengths. |
KI-1: I do hear all the girls talk about TV time not being healthy from the daycare. KI-2: They put in the walking trail, and I think they were trying to do a bike night in the community. I think those are good initiatives. . . . The longer it's here, the more people will think to do it. I think that the bigger towns really need to come up with ideas like that, and . . . better promote them or promote them longer. |
| PA barriers | |
| Competition with sedentary activities hinders PA. |
KI-3: There are too many kids that are sedentary because they're parked in front of the television or video box, and they are not getting enough exercise. KI-4: It's very difficult, especially when both adults or whatever adult you have in the home is tired, and it's just easier to let your kid watch TV or be on an iPad or computer or video game or something. |
| Suggestions | |
| Education and caregivers as positive role models are warranted. |
KI-10: I think we need to make people more aware of the options [meal preparation] that they could have [and] how they could fix some of those foods differently. KI-11: Specifically, [for children] 2–5 years of age, I think it starts in the home . . . I think it's up to us as adults to set better examples. |
| Note. PA = physical activity. | |
Caregiver Focus Group Session Results
Table 3 displays facilitator, barrier, and suggestion key concepts and supportive quotes from the caregiver focus group sessions for each topic area (healthful eating and PA).
| Key concept(s) | Supporting quotes |
|---|---|
| Healthful eating facilitators | |
| School policies and household rules combined with a supportive environment enable healthful food/beverage consumption. |
C-8: The Head Start where my little girl goes, they've done a lot of stuff on nutrition. Before, she loved pop. Now you can stick a bottle of water and a bottle of pop in front of her, [and] she will choose the water. C-9: In my house . . . if you want a snack, you have to eat a fruit or vegetable. You want to play with your electronics, well, you have to be outside for a while first. Because, otherwise, kids would do whatever they want. C-10: I've been to a couple, like, parties and things. It's always healthy snacks, vegetables with ranch dip, or something like that. |
| Healthful eating barriers | |
| Long distances to acquire healthful foods coupled with limited local availability, low quality, and cost pose challenges to healthful eating. |
C-11: I have to make a special trip, like 35 to 40 minutes, to get what we need in our house. C-12: The downfall about going to our grocery store here in town—we have one grocery store to choose from in the entire county—and if you buy a bag of apples or a bunch of bananas, you'd better eat them in the next day or two because they're going to go bad. The quality is very poor. C-13: Healthy food is expensive. It's 10 cents for a pack of ramen noodles. If you want to buy a bunch of bananas, you're looking at a lot of money, comparative. People on a fixed income, they just can't afford it. |
| Junk food is pervasive. | C-14: There's more exposure to junk food. My daughter is in pre-K, and she came home with a list of suggested snacks. And on the list of suggested snacks . . . were items like cheese puffs or Rice Krispies treats and cookies. |
| Time constraints inhibit healthful eating. | C-15: I think, as parents, we all want our children to eat well and healthy. Me, being a full-time [worker] . . . it's often hard to fit those in. . . . I believe that's why you see them visiting McDonald's drive-through [or] you see them at Pizza Hut after the game or after practice. |
| PA facilitators | |
| Children are learning new PA skills and have other unique opportunities for PA. |
C-1: Both my daughters know little pieces of yoga. And I've never done yoga in my life. They got that from somewhere. C-2: The college does provide those activities. It just did a local Olympics . . . I take my kids there, but there were maybe six younger kids from our community. They had so much fun. It was like the Olympics. They had these different stations set up. It was a physically active, nonstop 2 hours. |
| PA barriers | |
| Lack of sidewalks and PA opportunities hinder active living. |
C-3: There are no sidewalks all the way through town. It is quite annoying to try to walk. If I don't have a car and I am trying to walk to church, I can't walk on the sidewalk the whole way. You have to cross the highway multiple times to get to where you want to go because the sidewalks randomly end. C-4: There's nothing to do here besides put your kids in a sport. There's no skating rink. . . . We used to have swim nights on Tuesdays and Thursdays at the middle school pool. But that doesn't open until October. |
| Caregivers are inadequate role models. |
C-5: Parents are sitting in front of the television, and they're playing on the phone or their iPad or their tablet or their electronics. It's easier to give your kid a little iPad tablet, and they'll sit there next to you and not have a conversation [than to encourage them to] go outside and play. C-6: I've been watching the younger generation, and they're not as active as when we were their age. . . . They don't have the gumption—most of the ones I've run into—don't have the gumption to get up and go or do anything. |
| Communication is poor. | C-7: Those activities are already in place . . . if we don't know about them, we can't take advantage of them. |
| Suggestions | |
| Creative ideas include emphasizing the fun factor and creating a PA equipment reuse system. |
C-16: Make food fun, and make exercise fun. I mean, at that age, it has to be fun, or we are not going to have any. C-17: It would be really nice if there were open and active programs for hand-me-down stuff, for the soccer goal that your kid doesn't use anymore; 2- to 5-year-old [children] grow out of it so fast. C-18: They used to have a cooking class . . . and it was excellent. I miss it. . . . I learned to use some things that I would have never used in my home and didn't know how to use. My son, it was the best thing for him. He still asks about when we're going to have cooking classes again. |
| Note. PA = physical activity. | |
Examples of Themes Mapped onto the SEM
Examples of the themes (facilitators and barriers) were mapped onto an adapted SEM (Davison & Birch, 2001) to enable a visual representation at the various levels of the SEM. As can be seen in Figure 1, facilitators (+) and barriers (−) spanned multiple levels of the SEM and offered numerous points of potential intervention.
Figure 1.
Theme Examples and the Social Ecological Model
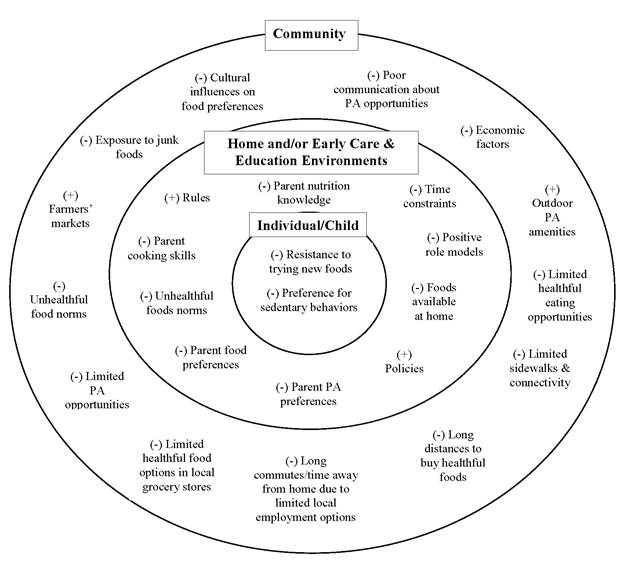
Note. PA = physical activity.
Community Action
The needs assessment yielded a rallying point around which rural communities can improve community environments for families with young children because it provided local critical contextual information. Community advisory committees (CACs), facilitated by the county-level Extension professionals on our team, were formed in each county. Each CAC was comprised of approximately 10 members who met quarterly to help plan and coordinate community-wide activities. CAC members represented a variety of sectors, including care giving, education, health, public office, and faith-based organizations. The county-level Extension professionals reviewed summaries of the needs assessment with their local CACs to help set priorities. We launched a health messaging campaign in each of the three counties, informed by Lanigan (2011), encouraging (a) daily consumption of a variety of fruits and vegetables, (b) active play every day, and (c) outdoor play. The messages were designed to combat the negative message environment identified in the needs assessment and to foreshadow messages that would be introduced as part of our childhood obesity prevention project in early care and education settings. CACs were actively engaged in distribution of messaging, including on billboards, grocery cart signs, and posters in health care settings.
CACs worked with us to implement a grant process for responding to identified needs. A total of 28 projects were funded, including projects involving
- natural playscapes,
- playground equipment enhancements geared toward young children,
- walking trails,
- garden-based learning,
- high tunnels,
- outdoor water fountains, and
- outdoor pavilions/learning centers.
These projects leveraged an additional $135,804 in the form of in-kind donations, labor, moneys from fundraisers and grants, and volunteer time, a 200% increase from the $65,000 invested through the initial funding process. Natural playscapes, which use the environment rather than prefabricated equipment to engage children, were a new concept for these communities. Over 50 volunteers came together and created play spaces out of plants, logs, and other natural elements to enable young children the opportunity to reap the health, developmental, and social benefits of outdoor play and exploration (Coe, Flynn, Wolff, Scott, & Durham, 2014; Peterborough Public Health, 2017). Each CAC also hosted a sustainability training and developed action plans to continue and expand these efforts after ending of the grant funding.
Limitations and Strengths
As with many qualitative inquiries, our sample size was small, limiting generalizability to other populations. Our coding process was thorough, given that after two coders independently coded all transcripts and resolved differences through consensus, a third person reviewed all codes for consistency. The inclusion of both key informants and caregivers to obtain a range of perspectives was another strength of our study (McKenna, Iwasaki, Stewart, & Main, 2011).
Discussion and Implications for Extension
Our needs assessment provided a community-level exploration of facilitators and barriers to promoting healthful eating and increasing PA among young children in rural communities. Both key informants and caregivers identified similar areas of concern about healthful eating. However, key informants and caregivers diverged in their perceptions about PA opportunities, with key informants indicating numerous opportunities but caregivers reporting limited opportunities and deficient communication about existing opportunities. Both groups identified barriers to healthful eating and PA for young children in rural and low-income communities similar to those identified previously in the literature. In particular, our findings support other research in rural communities suggesting interconnections among barriers—for example, the barrier of long distances to access food ties directly to the barrier of lack of time (Seguin et al., 2014).
Key stakeholders and caregivers in each of our project counties, facilitated by local Extension professionals, came together to address some of these barriers in order to improve the broader environment in which families with young children live and play. Providing local contextual data via our needs assessment facilitated this process. Collaborative efforts such as these, although sometimes lacking in rural areas, are essential to building a community's capacity to address obesity (Barnidge et al., 2013). The National Framework for Health and Wellness (Braun et al., 2014) encourages Extension professionals to engage with diverse sectors in their communities. Purposeful engagement of community members and volunteers by Extension professionals is recommended for empowering others to address community needs with local solutions (Washburn, 2017). The efforts described here can inform other Extension professionals working with rural communities.
Disclaimer and Acknowledgments
This publication was supported by Cooperative Agreement Number 5NU58DP005488-02-00 from the Centers for Disease Control and Prevention. Its contents are solely the responsibility of the authors and do not necessarily represent the official view of the Centers for Disease Control and Prevention.
We wish to thank the key informants and caregivers who gave their time and insights to our effort as well as all the volunteers who came out to improve the broader environments in which rural families with young children live and play.
References
Appalachian Regional Commission. (2017). Creating a culture of health in Appalachia—Health disparities and bright spots. Key findings West Virginia. Retrieved from https://www.arc.gov/images/appregion/fact_sheets/HealthDisparities2017/WVHealthDisparitiesKeyFindings8-17.pdf
Barnidge, E. K., Radvanyi, C., Duggan, K., Motton, F., Wiggs, I., Baker, E. A., & Brownson, R. C. (2013). Understanding and addressing barriers to implementation of environmental and policy interventions to support physical activity and healthy eating in rural communities. Journal of Rural Health, 29(1), 97–105.
Birch, L. L., Parker, L., & Burns, A. (2011). Institute of Medicine. Committee on Obesity Prevention Policies for Young Children. In Early childhood obesity prevention policies. Washington, DC: National Academies Press.
Bowen, E., Murphy, E., O'Hara-Tompkins, N., Crum, G., Fincham, H., & Burkhart-Polk, M. (2020). Early childhood obesity prevention in rural West Virginia: Extension's role and lessons learned. Journal of Human Sciences, 8(1), 163–177.
Braun, B., Bruns K., Cronk, L., Fox, L. K., Koukel, S., Le Menestrel, S., . . . Warren, T. (2014). Cooperative Extension's national framework for health and wellness. Retrieved from http://www.aplu.org/members/commissions/food-environment-and-renewable-resources/CFERR_Library/national-framework-for-health-and-wellness/file
Centers for Disease Control and Prevention. (2018). Overweight & obesity: Childhood obesity facts, 2018. Retrieved from http://www.cdc.gov/obesity/data/childhood.html
Coe, D. P., Flynn, J. I., Wolff, D. L., Scott, S. N., & Durham, S. (2014). Children's physical activity levels and utilization of a traditional versus natural playground. Children, Youth and Environments, 24(3), 1–15.
Cunningham, S. A., Kramer, M. R., & Narayan, K. M. (2014). Incidence of childhood obesity in the United States. New England Journal of Medicine, 370(5), 403–11.
Davison, K., & Birch, L. (2001). Childhood overweight: A contextual model and recommendations for future research. Obesity Review, 2(3), 159–171.
Fialkowski, M. K., DeBaryshe, B., Bersamin, A., Nigg, C., Guerrero, R. L., Rojas, G., . . . Novotny, R. (2014). A community engagement process identifies environmental priorities to prevent early childhood obesity: The Children's Healthy Living (CHL) program for remote, underserved populations in the US affiliated Pacific Islands, Hawaii and Alaska. Maternal and Child Health Journal, 8(10), 2261–2274.
Finkelstein, D. M., Petersen, D. M., & Schottenfeld, L. S. (2017). Promoting children's physical activity in low-income communities in Colorado: What are the barriers and opportunities? Preventing Chronic Disease, 14(2). Retrieved from https://www.cdc.gov/pcd/issues/2017/17_0111.htm
Harden, S. M., Gunter, K. B., & Lindsay, A. R. (2018). How to leverage your state's land grant Extension system: Partnering to promote physical activity. Translational Journal of the American College of Sports Medicine, 3(5), 113–118.
Hessler, K. L. (2009). Physical activity behaviors of rural preschoolers. Pediatric Nursing, 35(4), 246–253.
Johnson, J. A., & Johnson, A. M. (2015). Urban–rural differences in childhood and adolescent obesity in the United States: A systematic review and meta-analysis. Childhood Obesity, 11(3), 233–241.
Lanigan, J. D. (2011). The substance and sources of young children's healthy eating and physical activity knowledge: Implications for obesity prevention efforts. Child: Care, Health and Development, 37(3), 368–376.
Leeman, J., Myers, A. E., Ribisl, K. M, & Ammerman, A. S. (2015). Disseminating policy and environmental change interventions: Insights from obesity prevention and tobacco control. International Journal of Behavioral Medicine, 22(3), 301–311.
McKenna, S. A., Iwasaki, P. G., Stewart, T., & Main, D. S. (2011). Key informants and community members in community-based participatory research: One is not like the other. Progress in Community Health Partnerships, 5(4), 387–397.
Murriel, A. L., Kahin, S., Pejavara, A., & O'Toole, T. (2020). The High Obesity Program: Overview of the Centers for Disease Control and Prevention and Cooperative Extension Services efforts to address obesity. Preventing Chronic Disease, 17, 190235.
Peterborough Public Health. (2017). Outdoor play spaces: An evidence review. Retrieved from https://www.peterboroughpublichealth.ca/wp-content/uploads/2018/05/2017-08-31-Outdoor-Playspaces-Evidence-Report-FINAL-1.pdf
Sallis, J. F., & Owen, N. (2015). Ecological models of health behavior. In K. Glanz, B. K. Rimer, & K. Viswanath (Eds.), Health behavior: Theory, research, and practice (5th ed., pp. 43–64). San Francisco, CA: Jossey-Bass.
Seguin, R., Connor, L., Nelson, M., Lacroix, A., & Eldridge, G. (2014). Understanding barriers and facilitators to healthy eating and active living in rural communities. Journal of Nutrition and Metabolism, Article ID 146502. Retrieved from https://www.hindawi.com/journals/jnme/2014/146502/
Smathers, C. A., & Lobb, J. M. (2015). Extension professionals and community coalitions: Professional development opportunities related to leadership and policy, system, and environment change. Journal of Extension, 53(6), Article v53-6a1. Available at: https://www.joe.org/joe/2015december/a1.php
Smathers, C. A, Toomey, M., Washburn, L., Johnston, K., Iaccopucci, A. M., Johannes, E., & Ravola, M. (2019). Positive youth development for health: Extensions' readiness for multilevel public health approaches. Journal of Extension, 57(1), Article v57-1a1. Available at: https://www.joe.org/joe/2019february/a1.php
U.S. Department of Agriculture Farm Service Agency. (2014). Farm Bill Home. Retrieved from https://www.fsa.usda.gov/programs-and-services/farm-bill/index
Washburn, L. (2017). Engagement of health volunteers: A promising approach for meeting community needs. Journal of Extension, 55(3), Article v55-3comm1. Available at: https://www.joe.org/joe/2017june/comm1.php