August 2020
|
August 2020 // Volume 58 // Number 4 // Commentary // v58-4comm1




Commentaries conform to JOE submission standards and provide an opportunity for Extension professionals to exchange perspectives and ideas.
Activating Volunteers for Statewide COVID-19 Pandemic Response
Abstract
Extension is known for facilitating local networks and having the capacity to organize and mobilize volunteers. These assets, critically important in crises and emergency situations, were drawn on to support Tennessee's response to health care worker and community needs early in the coronavirus pandemic. Using local networks, we rapidly activated a statewide volunteer workforce to address potential shortages of cloth face masks before federal agencies recommended their widespread public use. We share social media communication strategies and a timeline of key events and acknowledge challenges we encountered in moving forward in an environment of inconsistent and evolving guidelines. Our actions may be applicable to addressing ongoing community needs as the pandemic persists and new circumstances arise.
Community engagement and coordinated action are hallmarks of the Extension system, which is known for facilitating local networks and having the capacity to organize and mobilize volunteers. Because of these strengths, particularly in crisis and emergency situations, Extension has been called on to provide leadership in assisting citizens and local governments in wartime and natural disasters (Black, 2012; Cartwright, Case, Gallagher, & Hathaway, 2002; Cathy, Coreil, Schexnayder, & White, 2007; Kelsey & Hearne, 1949).
In Tennessee, Extension's coronavirus pandemic response has been supported by members of Family and Community Education (FCE) clubs or Extension Homemakers Councils (EHCs), previously known as home demonstration clubs. With a stated mission of "strengthening individuals, families, and communities through continuing education, developing leadership and community action," the National Association for Family and Community Education is comprised of affiliated state organizations, each with county-based councils and clubs (National Association for Family and Community Education, 2019, "National FCE Mission"). Members of these groups have been consistent Extension allies through the years, most notably when engaged to support mattress-making efforts for poor families during World War II (Dean & Powers, 2014; Horton & Shelton, 1940; Meador, 2011; Wilson, n.d.). We describe how Extension personnel, hardwired to help in a crisis, activated this statewide volunteer workforce to meet pressing health care provider and community needs. Despite uncertainty, unclear science, and evolving guidelines, Extension agents, specialists, and volunteers organized with urgency to address a simple but important need: a potential face mask shortage for local health care workers. The actions we took early in Tennessee may serve as examples of ways to address community needs as the pandemic persists and new circumstances arise.
Situation
In early March 2020, the coronavirus and COVID-19 had become serious concerns across the country. Americans were advised to "flatten the curve" by social distancing, practicing diligent handwashing, and staying home (Qualls et al., 2017). Local and state governments closed nonessential businesses. By mid-March, Extension offices were closed, employees were working remotely, and programs were reimagined for virtual delivery.
Shifting to remote work disabled some traditional outreach methods. Extension agents grappled with remaining connected to their communities and were concerned about health issues stemming from loneliness and social isolation, particularly among older adults comprising a majority of the volunteer base (Holt-Lunstad, 2018). Opportunities to give and receive social support are a key benefit of FCE involvement. This support was restricted when needed most, increasing risk of emotional distress, anxiety, and depression (Usher, Bhuller, & Jackson, 2020).
While local Extension personnel were determining how to respond to needs and maintain physical distance, health care workers were growing concerned about personal protective equipment (PPE) supplies and possibilities of a severe shortage. The Centers for Disease Control and Prevention (CDC) advised use of homemade face masks as a last resort for those caring for COVID-19 patients, cautioning that homemade masks are not considered PPE (CDC, 2020a). Two members of our author team received initial health care worker requests for assistance in securing PPE and cloth face masks, prompting project initiation. The Extension community health specialist on our team was an advisor for the project.
What We Did
Requests for assistance were routed to county-based family and consumer sciences (FCS) Extension agents. As FCE advisors, agents recognized the potential dual positive impact of volunteer involvement in sewing cloth face masks. Beyond helping local health care workers, matching volunteers' sewing skills with pressing needs provided opportunity for the volunteers to contribute and find meaning in the coronavirus crisis, allowing for connection with others working toward common goals. Sewing, once part of FCS and 4-H but displaced in part by competing priorities for Extension programming, was reinitiated into a cadre of life skills promoted through Extension.
Work begun in two middle Tennessee counties quickly spread, as health care workers in other counties voiced mask needs. Early adopting agents promptly coordinated with a campus-based Extension specialist to jointly determine a course of action for engaging counties and volunteers statewide in addressing local needs for cloth face masks. A project coordination tip sheet and standardized mask patterns were distributed to Extension agents by email. Guidelines and recommendations on coordinating county-level projects were provided via a Zoom meeting.
A Facebook group created for the project, TAFCE Masks of Love Volunteers, was the primary channel for ongoing project communication. This group served three purposes: (a) facilitate consistent communication, (b) ensure quick response to questions and requests, and (c) connect Extension agents with others in their counties involved in sewing masks, including non-FCE members and 4-H youths and volunteers. A section was created for each county, showing agent contact information, pattern being used (if local providers requested deviation from the standard pattern), and other county-specific information. Troubleshooting help, daily sewing tips, and highlights such as posts including images of socially distanced mask deliveries were shared. To collect impact data, we created an online survey shared with Extension agents via email and volunteers via the Facebook group.
Results
Mask-making efforts involved 49 Tennessee counties, more than half of the counties in the state (see Figure 1). Volunteers contributed 21,178 hr in producing more than 22,551 masks. The value of this volunteer time is an estimated $538,557 (Independent Sector, 2018). Volunteers included FCE members, 4-H members, adult 4-H volunteers, and community volunteers not formally affiliated with Extension. With more than 850 members, the TAFCE Masks of Love Volunteers Facebook group fostered camaraderie and engagement. The group had 518 posts, 2,609 comments, and 10,951 reactions in less than 9 weeks.
Figure 1.
Map of Participating Tennessee Counties
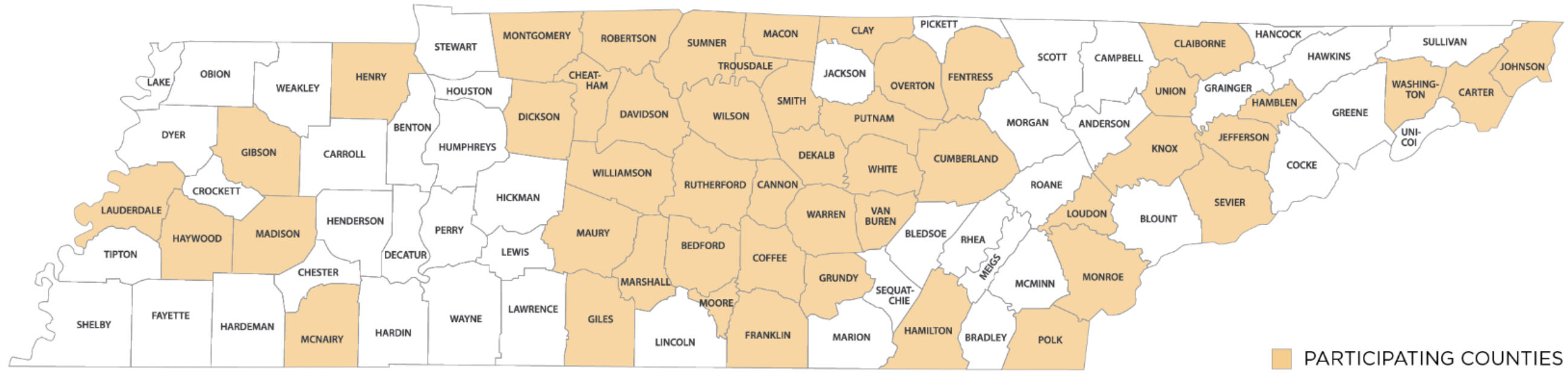
Face masks in most counties benefited local hospitals, health care facilities, or emergency services agencies. A number of community partnerships were developed, with outreach extending to school food service workers, postal workers, nursing homes, corner stores, county government, churches, mental health facilities, and law enforcement.
Eliciting expansion beyond the efforts to meet local needs, university leaders requested that volunteers assist with providing masks to essential employees working to conduct ongoing research activities and provide essential services, such as emergency veterinary care. This work was coordinated across counties, and masks were provided to 10 agriculture research facilities. Additionally, university and Extension leaders encountered supply chain issues in securing masks for employees as closed offices prepared for reopening; therefore, Extension agents leading the initiative coordinated production of 1,500 additional masks for on-campus and county Extension office employees.
Choosing Action in Uncertain Times
Operating with incomplete or imperfect information is inherent in emergencies and crises but is uncomfortable for those in a system that values research and science. In referencing Extension's role in emergencies, Kelsey and Hearne (1949) stated, "Speed is the important element of action" (p. 100). When incomplete information informs emergency response, acting before conventional standards of evidence are met may be required (Nash, Brown, & Cascio, 2020). Intervention in a crisis cannot aim for perfect deployment. Scientific accuracy may be impossible or even irrelevant to the response. The purpose of responding in crises is to meet community needs using the best available information. This requires balancing unknown and known factors. Here we describe several situational factors influencing consideration of potential costs and benefits of action versus inaction and measures to minimize risk.
Evolving Guidelines
Evolving information about the utility of cloth masks was a challenge to project messaging. The CDC issued guidance about use of homemade masks in health care settings in crisis situations where supply of PPE was running low (CDC, 2020a). The agency did not recommend widespread use of cloth face masks early in the pandemic, although masks are now recognized as effective in preventing COVID-19 infection (Zhang, Li, Zhang, Wang, & Molina, 2020). First priority was supplying masks for health care workers. To avoid misunderstandings, we explicitly stated in communication with volunteers and Extension agents that masks being made were not PPE and did not offer the protection of an N95 mask.
More than a month passed between our sharing of information for crisis use of homemade masks in health care settings and CDC recommendations for the general public to wear cloth face coverings when social distancing measures are difficult to maintain (CDC, 2020b). The mask-making project was widely adopted at that point (see Figure 2). Delaying the project by 1 month while waiting for recommendations or validation of cloth mask usefulness would have significantly slowed our response. We chose to forge ahead in the absence of clear guidance, solely in response to needs expressed by local health care providers that we were equipped to meet. Moving ahead to coordinate construction of cloth face masks was a low-risk endeavor and could potentially benefit others. Delaying action in hopes of clear guidance also may have been low risk, but for a service-oriented organization, the benefits of moving forward in a crisis outweighed concerns.
Figure 2.
Timeline of Key Events, 2020
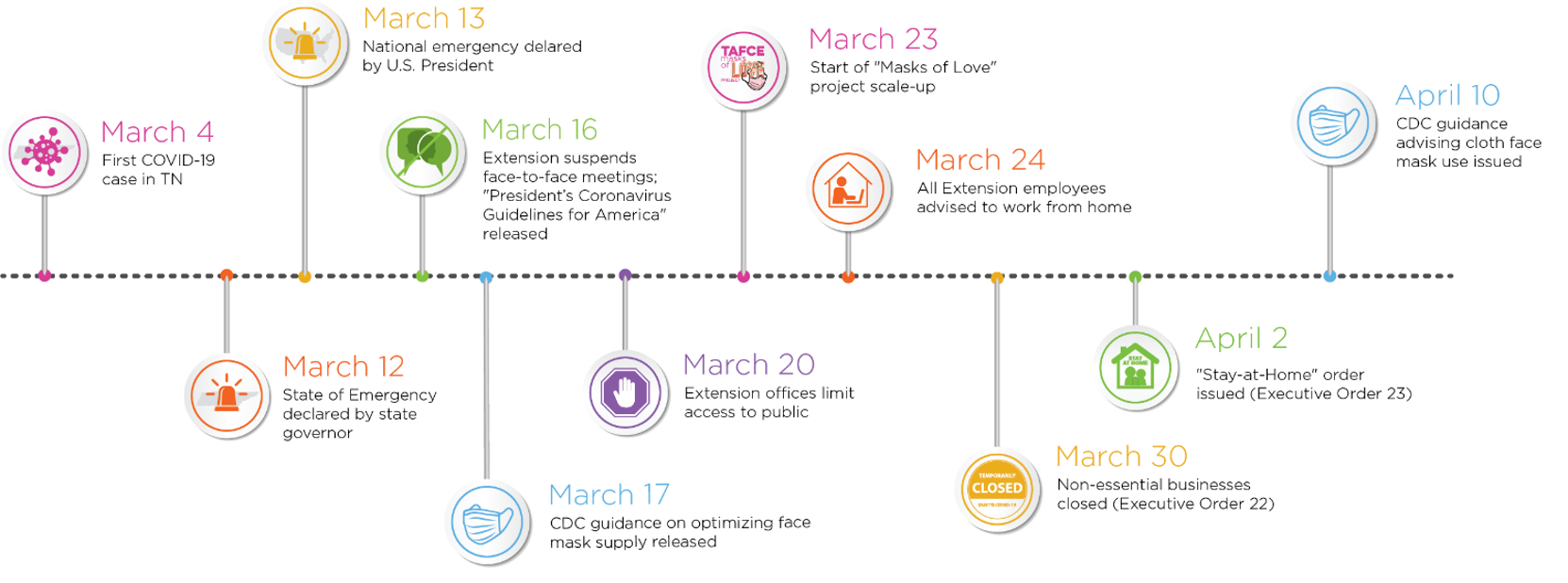
Note. CDC = Centers for Disease Control and Prevention.
Adjusting Strategy for Social Distancing
One week after statewide project scale-up, state government closed nonessential businesses and encouraged residents to stay home. A revised order requiring residents to stay home unless engaging in essential activities or services followed (Tenn. Exec. Order No. 22, 2020; Tenn. Exec. Order No. 23, 2020). Many volunteers and some Extension personnel were part of "high risk" groups. Ensuring safety, practicing social distancing, and promoting compliance with stay-at-home orders was of primary concern and potentially in conflict with the mission to continue making masks and procuring needed supplies. Quick, clear communication via email and Facebook provided direction to ensure volunteer and Extension personnel safety. No-contact "porch pick-up" of completed masks and distribution to facilities was coordinated.
Local Coordination and Connections
The project was coordinated locally, although general guidance was drafted and disseminated from the state level. From early in the project, communication of guidelines and recommendations was clear, consistent, and frequent (McAllister & Hilt, 2002). We relied on Extension agents to promote and coordinate work, starting with contacting local health care providers to determine mask needs and then communicating needs to volunteers.
Conclusion
Quick activation of networks connecting volunteers with health care providers demonstrated that Extension remains tightly woven into the community fabric. Community involvement benefited volunteers' mental health in a period of limited social interaction. This public health crisis highlighted within the Extension system a latent agility for quick response and demonstrated social media use as a tool in implementing large-scale Extension outreach efforts. Effective crisis response relies on relationships. Our efforts may serve as examples of ways to address ongoing community needs as the pandemic persists and new circumstances arise. Moreover, as noted by Nash et al. (2020) and reinforced by our experience, strengthening networks and developing leaders in noncrisis times positions Extension to act in the next emergency, disaster, or crisis.
Acknowledgments
Special thanks to Cris Miramontes for graphic design assistance and creation of figures.
References
Black, L. (2012). Disaster preparedness and the Cooperative Extension Service. Journal of Extension, 50(3), Article v50-3comm1. Available at: https://joe.org/joe/2012june/comm1.php
Cartwright, S., Case, P., Gallagher, T., & Hathaway, R. (2002). Extension's role in responding to community crisis: Lessons from Klamath Falls, Oregon. Journal of Extension, 40(6), Article 6FEA2. Available at: https://www.joe.org/joe/2002december/a2.php
Cathy, L., Coreil, P., Schexnayder, M., & White, R. (2007). True colors shining through: Cooperative Extension strengths in times of disaster. Journal of Extension, 45(6), Article 6COM1. Available at: https://www.joe.org/joe/2007december/comm1.php
Centers for Disease Control and Prevention. (2020a). Strategies for optimizing the supply of facemasks. Retrieved from https://www.cdc.gov/coronavirus/2019-ncov/hcp/ppe-strategy/face-masks.html
Centers for Disease Control and Prevention. (2020b). Use of cloth face coverings to help slow the spread of COVID-19. Retrieved from https://www.cdc.gov/coronavirus/2019-ncov/prevent-getting-sick/diy-cloth-face-coverings.html
Dean, V. W., & Powers, R. (2014) "In no way a relief setup": The county cotton mattress program in Kansas, 1940–1941. Kansas History: A Journal of the Central Plains, 37, 242–255. Retrieved from https://www.kshs.org/publicat/history/2014winter_dean.pdf
Holt-Lunstad, J. (2018). The potential public health relevance of social isolation and loneliness: Prevalence, epidemiology, and risk factors. Public Policy & Aging Report, 27(4), 127–130. doi:10.1093/ppar/prx030
Horton, M., & Shelton, J. (1940). The cotton mattress demonstration program in Texas (Publication No. B-119). The Extension Service Agricultural and Mechanical College of Texas and the United States Department of Agriculture. Retrieved from https://oaktrust.library.tamu.edu/bitstream/handle/1969.1/156627/Bull0119a.pdf?sequence=16
Independent Sector. (2018). Value of volunteer time. Retrieved from https://independentsector.org/value-of-volunteer-time-2018/
Kelsey, L. D., & Hearne, C. C. (1949). Cooperative Extension work. Ithaca, NY: Comstock Publishing Company.
McAllister, D., & Hilt, M. (2002). Sound internal communication is crucial in a crisis situation. Journal of Extension, 40(4), Article 4TOT2. Available at: https://www.joe.org/joe/2002august/tt2.php
Meador, M. (2011). Extension Homemaker Clubs. Retrieved from https://www.wvencyclopedia.org/articles/2223
Nash, A., Brown, S. C., & Cascio, J. (2020). Importance of best guesses in emergency situations. Journal of Extension, 58(3), Article v58-3comm2. Available at: https://www.joe.org/joe/2020june/comm2.php
National Association for Family and Community Education. (2019). National Association for Family and Community Education. Retrieved from https://www.nafce.org/
Qualls, N., Levitt, A., Kanade, N., Wright-Jegede, N., Dopson, S., Biggerstaff, M., . . . Uzicanin, A. (2017). Community mitigation guidelines to prevent pandemic influenza—United States, 2017. Morbidity and Mortality Weekly, 66(1), 1–34.
Tenn. Exec. Order No. 22 (March 30, 2020). An Order Directing Tennesseans to Stay at Home Unless Engaging in Essential Activities to Limit Their Exposure to and Spread of COVID-19. Retrieved from http://publications.tnsosfiles.com/pub/execorders/exec-orders-lee22.pdf
Tenn. Exec. Order No. 23 (April 2, 2020). An Order Amending Executive Order No. 22, Requiring Tennesseans Stay Home Unless Engaging in Essential Activity or Essential Services. Retrieved from https://publications.tnsosfiles.com/pub/execorders/exec-orders-lee23.pdf
Usher, K., Bhullar, N., & Jackson, D. (2020). Life in the pandemic: Social isolation and mental health. Journal of Clinical Nursing, 29(15–16), 2756–2757. https://doi.org/10.1111/jocn.15290
Wilson, L. D. (n.d.). Home demonstration clubs. Retrieved from https://www.okhistory.org/publications/enc/entry.php?entry=HO020
Zhang, R., Li, Y., Zhang, A. L., Wang, Y., & Molina, M. J. (2020). Identifying airborne transmission as the dominant route for the spread of COVID-19. Proceedings of the National Academy of Sciences, 17(26), 14857–14863. doi:10.1073/pnas.2009637117