October 2019
|
October 2019 // Volume 57 // Number 5 // Feature // v57-5a1



Engaging Residents in Participatory Photomapping and Readiness Conversations to Address the Rural Obesogenic Context
Abstract
Extension engaged rural Idaho community stakeholders to assess local resources and readiness to address obesogenic contexts through use of the Extension tool HEAL MAPPS. Through participatory photomapping, focus group involvement, and a community readiness conversation, residents identified environmental resources and local efforts as supports for and barriers to healthful eating and active living. Findings indicated that the community was "vaguely aware" that rural obesity risk is a socioenvironmentally determined issue. Extension professionals using HEAL MAPPS effectively promoted new and shared knowledge of weight health resources among community members, enabled rural residents to have a voice in addressing the community context, and empowered community actions.
Introduction
Overweight and obesity, presenting in childhood and leading to obesity in adults (Gordon-Larsen & Adair, 2010), have been universally established as among the most critical public health issues in the United States. In 2015–2016, the prevalence of obesity was 18.4% in youths aged 6–11 years and 20.6% in adolescents aged 12–19 (Hales, Carroll, Fryar, & Ogden, 2017). Moreover, rural residency tends to increase obesity risk: Children living in rural compared to metropolitan areas are 25% more likely to be overweight or obese (U.S. Department of Health and Human Services Health Resources and Services Administration, 2014). Rural overweight children are more likely to be female, to live in low-income households, and to be sedentary (due to screen time) for 3 hr or more per day (Lutfiyya, Lipsky, Wisdom‐Behounek, & Inpanbutr‐Martinkus, 2007). Weight-healthful lifestyles, specifically those in which healthful dietary behaviors are balanced with daily physical activity (PA), help prevent obesity.
Over the past decade, a growing evidence base has demonstrated the environmental correlates of obesity, including those specific to the rural community context (Boehmer, Lovegreen, Haire-Joshu, & Brownson, 2006). Public health scientists have contended that policy, systems, and environmental (PSE) interventions targeting obesogenic features to which people are regularly exposed may reduce the prevalence of obesity in populations (Boehmer et al., 2006). Identifying community features experienced as obesogenic, specifically the local features that make obesity-preventing lifestyle behaviors difficult for many, may be useful for guiding PSE interventions. In previous studies, Extension professionals have successfully used community-based participation methods to collect information on community needs (e.g., Seeger, Lillehoj, Jensen, Wilson, & Levinson, 2014). Extension researchers with Oregon State University's GROW Healthy Kids and Communities initiative (GROW) developed participatory action research (PAR) tools to engage rural residents in exploring and improving the obesogenic contexts where they live (John, Gunter, Hystad, Langellotto, & Manore, 2016).
GROW was funded as an integrated research, education, and Extension multistate collaboration by the U.S. Department of Agriculture under its childhood obesity prevention program (John et al., 2016). The community project we report here as a case study was directed through GROW's collaboration with Extension in six western U.S. states to identify features of individual rural communities that are experienced by residents as obesogenic environmental determinants hindering healthful eating and active living (HEAL) for families with children. To engage Extension audiences in community needs assessments aimed at improving local HEAL contexts, GROW investigators developed and trademarked Mapping Attributes using Participatory Photographic Surveys, or HEAL MAPPS, a PAR tool for mapping community resources and assessing readiness to address obesogenic features (John et al., 2017). In Extension, identifying different and easily available technologies (e.g., use of GPS or Google Earth) for producing valid data on local communities can lead to accessible, credible information for communities and additional opportunities for outreach and education (Huff, 2014).
HEAL MAPPS, nationally disseminated via the SNAP-Ed Toolkit (https://snapedtoolkit.org/interventions/programs/heal-mapps/), is a theoretically modeled, evidence-based strategy effective for mobilizing community change. Through HEAL MAPPS, residents are involved in participatory photomapping and storytelling related to their experiences of local environmental supports for and barriers to their families' healthful eating and PA patterns (John et al., 2017). The process includes intentionally recruiting residents who represent the local demographic diversity to participate in every aspect of the study; these respondents help identify a variety of lived experiences and share diverse perceptions about the local community HEAL context (John et al., 2017). Additionally, the community readiness model (CRM) (Oetting et al., 2014) is integrated into HEAL MAPPS, allowing for scaling of the community's readiness to improve the local HEAL context as a socioenvironmental approach to minimizing obesity risk among residents. The CRM includes six dimensions that are community issue–specific: resources, current efforts, knowledge of efforts, knowledge of issue, leadership, and climate. Evaluating community readiness encompasses applying a 9-point scale (1—no awareness through 9—community ownership) to observable qualities applicable to each dimension. This component of HEAL MAPPS is essential, as community readiness is a major factor in determining whether a community can support, adopt, and successfully implement a program addressing an issue.
The prevalence of obesity in Idaho has increased significantly in recent years, with approximately three in 10 adults and one in 10 children categorized as obese (Robert Wood Johnson Foundation, n.d.). The 2018 National Health Statistics Report showed that only 31.4% of adults aged 18–64 in Idaho met the 2008 federal guidelines for both aerobic and muscle-strengthening activities (Blackwell & Clarke, 2018, p. 5), and about one in five Idaho adults report no participation in leisure time PA (Idaho Department of Health and Welfare Division of Public Health, 2014, p. 8). Rural communities differ from one another in many ways, including regarding resources and readiness to take action on obesogenic issues and implement relevant PSE interventions. University of Idaho (UI) Extension, in partnership with and supported by GROW, adopted the HEAL MAPPS program. In this case study report, we describe how HEAL MAPPS was used in one rural community to mobilize residents to assess the community's HEAL resources and readiness capacity. Community-informed findings provided data for collaboratively planning and implementing PSE interventions and tracking community changes. Findings were relevant to the case study community, but more broadly speaking, our experiences with HEAL MAPPS are relevant to Extension professionals working elsewhere to address the socioenvironmental determinants of obesity among residents of rural locales. Additionally, the case study mechanism could be applicable to addressing other community health issues (John & Gunter, 2016) and relevant as those in rural areas of states implement the Cooperative Extension National Framework for Health and Wellness (Braun et al., 2014).
Methods
A team of UI Extension educators, including authors Jensen and Tifft, participated in a 20-hr train-the-trainer workshop delivered by authors Winfield and John, who led HEAL MAPPS program development. Within 1 month of the team training, authors Jensen and Tifft (hereafter referred to as "the Extension educators"), who are based in north-central Idaho, partnered with a community concerned about obesity risk to implement HEAL MAPPS. After identifying a local champion as a first step, the Extension educators worked closely with the community champion to recruit community partners and stakeholders, including local organizations and residents, as participants and implemented HEAL MAPPS activities according to protocol. Specifically, Extension trained and mobilized community stakeholders to (a) photomap community resource availability and residents' experiences of resource accessibility, (b) facilitate residents' identification of key resources, (c) enable discussion from diverse perspectives, and (d) report HEAL resources and community readiness findings that informed local recommendations for action (John et al., 2017).Participants
The Extension educators worked closely with the community champion and sector stakeholders to recruit adult residents representing the income, age, and gender diversity of the community's family households with children to participate in study activities. With the help of sector stakeholders, the Extension educators assembled and mobilized a volunteer team of nine community residents with interest in child obesity prevention to assess the community's HEAL context by photomapping accessibility experiences with locally available HEAL resources.
Data Collection
The Extension educators facilitated HEAL MAPPS community-engaged data collection activities. Three types of data collection activities occurred over a 6-week time period and are described in Table 1. The Extension educators worked closely and cooperatively with the community PAR team and with the GROW research team to assure that data were collected and managed with fidelity to HEAL MAPPS protocol. For example, the Extension educators recruited and trained two volunteer scribes who attended the community conversation activity purposely to collect the narrative data generated during the conversation. During this activity, individual scribes took detailed notes throughout the community conversation, writing the discussion verbatim and recording the percentage scores from audience polls. Within a day or two of the activity, the Extension educators worked with the scribes to combine their individual notes pages for each slide into one community conversation transcript. The Extension educators were responsible for secure, electronic transfer of all field data generated via the three collection activities, including GPS data files (geo-coded photographs and route map location data), scanned mapper worksheets, electronic poll data, and verbatim transcription documents, to the GROW research team for managing.
| Data collection activity | Description | Data outputs |
|---|---|---|
| Residents' photomapping |
Extension educators trained and deployed the recruited residents to photomap. These community "mappers" collected data using camera-enabled GPS units (provided) to photograph, and thus map, the community food and PA resources they accessed regularly. Mappers, working individually, logged their access experiences using HEAL MAPPS photo journal worksheets (provided). Mappers wrote comments specific to each photographed resource to provide reasons for their ratings of whether a resource made "eating healthfully" and/or "being physically active" most every day "easy" or "hard" for themselves and their families. Extension educators collected the GPS units and worksheets from the mappers within 2 weeks of the training. |
Mappers (n = 9) produced 130 resource photographs, mapped and logged (e.g., as easy or hard and why) along nine routes covering 61 linear road miles representing the community's active (e.g., walking, bicycling) and motor vehicle transportation system used to access the community's available HEAL resources. |
| Mapper focus group session |
Extension educators reconvened mappers as a focus group to review their data—resource photographs and route map locations. Mappers, through group consensus, determined which subset of photographs best represented the community's HEAL attributes. |
Mappers selected 79 unique photographs of local food and/or PA resources as data representative of the community HEAL context. |
| Community conversation |
Extension educators, working with stakeholders to broaden community reach, advertised an open invitation to a community dinner and group discussion facilitated according to HEAL MAPPS protocol. Adult residents and other sector stakeholders (i.e., elected officials, school personnel, and business owners) participated in the Extension-facilitated HEAL community conversation. Extension educators displayed slides with images of photographed features and encouraged attendees to actively view the slides, discuss the photographed community resources, and voice their perceptions and polled opinions in order to generate and collect new data. Attendees used audience response system clickers (provided) to respond anonymously. Polled opinions, quantified as percentages per response option, were immediately displayed on the poll slide. Extension educators further encouraged participants to voluntarily voice thoughts and feelings that had led to their opinion ratings, such as why they perceived that a displayed feature made it easy (extremely, somewhat) or hard (somewhat, extremely) for them or others in the community to eat healthfully or be physically active. |
Audience members (n = 22) discussed the displayed resource photographs as they were viewed and responded to CRM poll questions associated with photographs of representative resources, producing opinion poll data and conversation narratives for further documenting the community's HEAL context and indicators of resources, readiness, and capacity for change. |
| Note. CRM = community readiness model. HEAL = healthful eating and active living. PA = physical activity. | ||
Data Analysis
Led by authors Winfield and John, "GROW evaluators" conducted the data analysis. GROW evaluators are members of the GROW research team who have expertise in HEAL MAPPS data sources, data collection, and mixed-methods (quantitative and qualitative) design. The GROW evaluators' analyses were confirmed by the Extension educators, who were members of the community PAR team. The GROW evaluators coded data from all community sources—photos, photo journals, route maps, and transcriptions of the community conversation—into "healthful eating" and "physically active living" thematic categories as well as into six HEAL-adapted CRM dimensions (i.e., HEAL-specific resources, current efforts [supports, barriers], knowledge of efforts, knowledge of HEAL issues, leadership, and climate). Two GROW evaluators assessed community HEAL readiness in each dimension by following CRM protocol and applying the 9-point rating scale embedded in the HEAL MAPPS program. The score for each dimension could range from 1 to 9. Protocol required that discrepancies between two evaluators' scores of greater than 1 point in any dimension be resolved by a third expert evaluator (author John, a GROW principal investigator). The expert evaluator, who also provided reliability checks on 20% of all coded data, independently rated the dimension in question to provide a reliable base score. The GROW evaluators averaged the scores for the six CRM dimensions to produce an overall community readiness score. The Extension educators used a HEAL MAPPS template to develop a community-specific report into which results, including local HEAL resources, readiness dimensions, and overall community readiness scores, were integrated by the GROW evaluators (Jensen, Tifft, Winfield, Gunter, & John, 2016). Reported findings were confirmed locally by the case study community's PAR team with the facilitative help of the Extension educators.
Results
Analyses and interpretation conducted by the GROW research team merged concurrent data from all sources across the three sequential data collection activities occurring during the HEAL MAPPS implementation; the sources were photographs, journal entries, mapped routes and locations, poll results, and narratives. Data triangulation across activities revealed that community members' experiences of place-based resources varied in terms of being HEAL supporting or HEAL obstructing (see Table 2), although the polling data revealed that most (73%) disagreed that the community had adequate resources to help a variety of community members eat healthfully and be physically active. Additionally, according to the poll results, only about one in four residents (27%) were moderately or very knowledgeable about the "link between the community environment and obesity risk." Most residents polled (95%) felt that child obesity was an issue of concern "in their community." The majority (89%) felt that community leaders were not at all or only mildly engaged "in efforts to promote weight healthy kids and families." Everyone responding to the poll (100%) was either absolutely (50%) or moderately (50%) willing to work for changes in the community place to make it easier for all children and families to eat healthfully and be physically active most every day.
| Resource |
Support (makes HEAL easy) |
Barrier (makes HEAL hard) |
|---|---|---|
| Healthful eating | ||
| Grocery stores/markets | Available variety of healthful and fresh local food; health food store | Low number of retailers accepting SNAP benefits (food stamps) (i.e., one market only) |
| Local agriculture—farmers' markets, farm stands, produce retailers | Cottage food laws; local animal- and plant-based products—meat, eggs, dairy/cheese, produce | Inefficient marketing and communication technologies and information reach |
| Prepared convenience/fast foods | Some healthful options; few fast food choices | No grab-n-go healthful options; convenient unhealthful snacks |
| Prepared restaurant/café foods | Availability of more healthful and vegetarian options; nutrition information on menus | |
| Educational programs | Availability of programs (e.g., Eat Smart Idaho, Grub Club), events (e.g., Wellness Fair, Heart Walk), and information | Inaccessible (e.g., due to distance) or exclusive (e.g., due to age, income) settings, hours, locations of classes |
| Food assistance—meals and pantries | Availability and food quality (e.g., from-scratch, RD-approved delivered meals) and quantity (2 meals); some all-serving sites (e.g., senior center) | Inaccessible (e.g., due to distance) or exclusive (e.g., due to age, provider), settings (e.g., church), hours, locations; food quality (e.g., low-cost packaged foods) |
| Schools | School meal programs that include breakfast and lunch | Lack of participation in school meals during summers/need for transportation for summer lunch participation; availability of sugary snacks/drinks |
| Physically active living | ||
| Community-based active recreation programs | Availability of variety of active recreation programs and events | Hard to sustain—low/seasonal enrollment and lack of public transportation, funding, and personnel for sustainability |
| Public parks/playgrounds | Availability of no/low-cost sports fields, courts, parks, playgrounds | Limited tax base for funding/maintenance of public spaces, bathrooms, equipment |
| Private/commercial fitness centers, sports centers, gymnastics/dance | Availability of multiple types of exercise/sports centers; some open to public (fee-based) | Costs of membership/user fees (unaffordable, excessively high) |
| Natural/outdoor (rural) landscape | Abundant natural/outdoor activity spaces (lakes, creeks, watershed, ski/tubing hills) | Inaccessible/incomplete/unsafe activity spaces/trails (i.e., car and time dependent due to distance, restrictive/private land-use policies, no shared/public use liability rule); equipment and clothing costs; dog and wildlife encounters |
| Built environment walkability/"bikeability" | Rails-to-trails to nearby town; ADA-accessible lake | Inadequate pedestrian/bicycle signage/safety; no bike racks; no/discontinuous and poorly maintained sidewalks and bike lanes |
| Schools | Available outdoor fields/courts, new outdoor track surface, indoor gym/ courts/climbing wall with limited community use | No liability agreement for indoor spaces; fee-based shared use for gym; poor lighting/maintenance of courts/equipment |
| Note. ADA = Americans with Disabilities Act. RD = registered dietician. SNAP = Supplemental Nutrition Assistance Program. | ||
Qualitative data coded into six a priori CRM dimensions were transformed into numerical scores ranging from 1 (no community awareness) to 9 (community ownership/professionalism) according to the CRM-criteria-anchored rating scale. Scores ranged from 3 (lowest) for "resources" to 4 (highest) for "current efforts" and "climate" related to the HEAL issue (see Figure 1). The overall community readiness score, which was calculated as the mean of the scores for the six dimensions, was 3.6, indicating that generally the community was between "vague awareness" and "preplanning" in terms of collective readiness to prioritize and implement community PSE strategies to increase supports for and reduce barriers to HEAL (see Figure 1).
Figure 1.
Scores for Six Dimensions and Overall Community Readiness to Improve the Healthful Eating and Active Living (HEAL) Environment
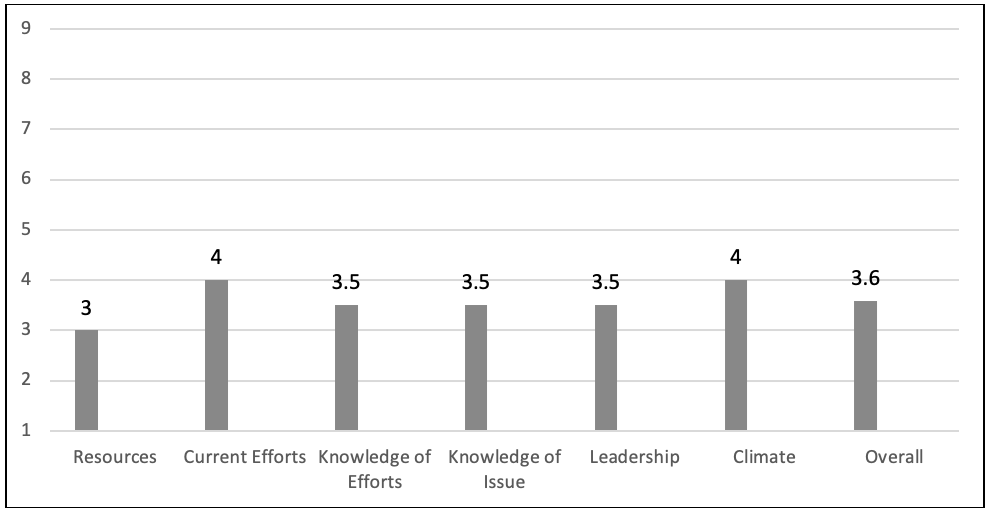
Note: 1 = no awareness, 2 = denial, 3 = vague awareness, 4 = preplanning, 5 = preparation, 6 = initiation, 7 = stabilization, 8 = expansion, 9 = community ownership
Discussion
Close collaboration and regular communication between the Extension educators and the GROW evaluators across all phases of data collection, analysis, and reporting was critical for assuring that knowledge generated and transferred about the community HEAL context was trustworthy, relevant, and accessible to the community. The HEAL MAPPS PAR approach can be seen as an innovation within Extension for determining and disseminating information among community leaders about issues revealed when working with community members.
HEAL MAPPS moved Extension from deliverer of information to enabler of local discovery and learning by involving the community directly in the collection and analysis of information through their "world view." The participants' rich, meaningful stories reflected their diverse lived experiences of the same HEAL features. For example, we learned that HEAL resource access was influenced by location relative to where family members resided, worked, or went to school. Despite the availability of three city parks located within the city limits, there were no bike lanes, and many streets had no sidewalks or had sidewalks that were unsafe, making it difficult for rural children and underresourced families to engage in regular PA.
The Extension educators provided a written report (Jensen et al., 2016) to the community stakeholders that included the community's data profile, readiness dimension scores and strategies, and locally determined recommendations for change. The Extension educators helped community action groups use PAR findings to outline next steps, prioritize actions, and secure resources to address the prioritized barriers. Within this rural community, use of HEAL MAPPS proved to be an efficient approach to meeting Extension's role as both community educator and evaluator. HEAL MAPPS can be an effective outreach and engagement strategy for Extension professionals working with communities to determine PSE intervention priorities and next steps for community action. Specifically, use of HEAL MAPPS can help Extension professionals and communities
- develop culturally tailored informational campaigns to increase knowledge of issue, efforts, and resources for HEAL;
- engage local leaders in efforts to plan and increase active living resources (e.g., safe and connected walking/biking trails/paths);
- apply an equity lens to new PSE intervention efforts to assure that HEAL resources are known, easily accessible to all, and sustainable; and
- increase multisector partnerships with shared goals as a resource for a HEAL community culture, and track local impacts.
Strength and Limitations
In the project described here, Extension educators successfully implemented HEAL MAPPS, a PAR approach to community-engaged education. The educators leveraged collaborative relationships with partners in social services, business, government, and nonprofits to engage communities and residents in the discovery process. Local knowledge and experiences were respected and valued in the mapping and categorizing of the information collected.
Nonetheless, in this case, limitations emerged during implementation of HEAL MAPPS. Engaging a diverse representation of community members was a challenge even with specific participation diversification strategies embedded in the program. Participant diversity would improve the trustworthiness of the findings as representative of the community's experiences with the resources and readiness to act. Increased diversity also would increase the relevance of the results beyond the participants and help establish the public value of Extension's efforts to promote HEAL community development. Further, engaging participants from all private and public sectors and demographic groups would assure that PSE resourcing decisions and actions are informed and understood by all stakeholders.
Conclusion and Implications
Many challenges that exist for rural family households with children are invisible, such as diverse family structures, commuting distances, unemployment/underemployment, HEAL resource deserts, and more. If solutions are truly to be equitable, and rural health disparities addressed, intention and attention by the research/academic and Extension community are required to assure that diverse voices are included and heard. Our HEAL MAPPS implementation enabled rural residents to have a voice and empower community actions based on what their community offered (supports) and did not offer (barriers) related to HEAL.
Extension educators are already key players in helping build community capacity. Embedded in communities, Extension has a current and historical understanding of unique community inequalities and a responsibility to meet community needs and benefit the greater good. Extension is also building internal capacity for employing emerging and innovative technologies that add value to our outreach. Using a community-engaged, research-based program, such as HEAL MAPPS, was effective for promoting new and shared knowledge of weight health resources and readiness for change among community members.
An aim of conducting the project reported here was to advance knowledge and community-level strategies of use to Extension educators. Extension programs involving evidence-based discovery tools, such as CRM, participatory photomapping, and community conversations, offer potential benefits to rural communities attempting to address local supports for healthful eating and active living.
The well-documented magnitude of the national obesity issue demonstrates the critical need for Extension to adopt new and effective strategies to minimize obesity risk factors. Because of our project in a rural Idaho locale, community members and leaders now share awareness that obesity is a social issue and are planning for new efforts that are cost-manageable, best-practice solutions. Providing options for and sustaining HEAL assets that help all adults and children develop healthful lifestyle habits strengthens our collective effort to reduce rural obesity risk and rates in Idaho and the nation.
References
Blackwell, D. L., & Clarke, T. C. (2018). State variation in meeting the 2008 federal guidelines for both aerobic and muscle-strengthening activities through leisure-time physical activity among adults aged 18–64: United States 2010–2015. (National Health Statistics Reports Report No. 112). Hyattsville, MD: National Center for Health Statistics.
Boehmer, T. K., Lovegreen, S. L., Haire-Joshu, D., & Brownson, R. C. (2006). What constitutes an obesogenic environment in rural communities? Journal of Health Promotion, 20(6), 411–421.
Braun, B., Bruns, K., Cronk, L., Fox, L., Koukel, S., LeMenestrel, S., . . . Warren, T. (2014, March). Cooperative Extension's national framework for health and wellness. Retrieved from https://www.aplu.org/document.doc?id=5134
Gordon-Larsen, P., & Adair, L. S. (2010). Longitudinal trends in obesity in the United States from adolescence to the third decade of life. Obesity, 18(9), 1801–1804. Retrieved from https://www.cdc.gov/obesity/childhood/causes.html
Hales, C., Carroll, M., Fryar, C., & Ogden, C. (2017). Prevalence of obesity among adults and youth: United States, 2015–2016. (Report No. 288). Retrieved from https://www.cdc.gov/nchs/data/databriefs/db288.pdf
Huff, T. (2014). Google Earth: Low-investment GIS for Extension professionals. Journal of Extension, 52(4), Article 4TOT2. Available at: https://www.joe.org/joe/2014august/tt2.php
Idaho Department of Health and Welfare Division of Public Health. (2014). Idaho health behaviors. Retrieved from http://www.healthandwelfare.idaho.gov/Portals/0/Health/Statistics/BRFSS%20Reports/Idaho_BRFSS_Annual_Report_2014.pdf
Jensen, K., Tifft, K., Winfield, T., Gunter, K., & John, D. (2016). Grangeville, ID. HEAL MAPPS community report. Retrieved from http://extension.oregonstate.edu/growhkc/sites/default/files/community_report_grangeville_final20161012.pdf
John, D., & Gunter, K. (2016). Engage in community: Mobilizing local people to elucidate the age-friendly attributes of place. Journal of Applied Gerontology, 35(10), 1095–1120.
John, D., Gunter, K., Hystad, P., Langellotto, G., & Manore, M. (2016). Generating rural options for weight healthy kids and communities—Outcomes and impacts. Journal of Nutrition Education and Behavior, 48(7), S122.
John, D., Winfield, T., Etuk, L., Hystad, P., Langellotto, G., Manore, M., & Gunter, K. (2017). Community-engaged attribute mapping: Exploring resources and readiness to change the rural context for obesity prevention. Progress in Community Health Partnerships: Research, Education, and Action, 11(2), 183–196. Retrieved from https://muse.jhu.edu/article/665059
Lutfiyya, M. N., Lipsky, M. S., Wisdom‐Behounek, J., & Inpanbutr‐Martinkus, M. (2007). Is rural residency a risk factor for overweight and obesity for U.S. children? Obesity, 15, 2348–2356. doi:10.1038/oby.2007.278
Oetting, E. R., Plested, B. A., Edwards, R. W., Thurman, P. J., Kelly, K. J., & Beauvais, F. (2014). Community readiness for community change: Tri-Ethnic Center community readiness handbook (2nd ed.). Retrieved from http://www.triethniccenter.colostate.edu/docs/CR_Handbook_8-3-15.pdf
Robert Wood Johnson Foundation. (n.d.). The state of obesity in Idaho. Retrieved April 15, 2019, from The State of Obesity website: https://www.stateofobesity.org/states/id/
Seeger, C. J., Lillehoj, C. J., Jensen, A. D., Wilson, S., & Levinson, L. R. (2014). I-walk: An innovative approach to community walkability. Journal of Extension, 52(4), Article 4IAW7. Available at: https://www.joe.org/joe/2014august/iw7.php
U.S. Department of Health and Human Services Health Resources and Services Administration. (2014). The health and well-being of children: A portrait of states and the nation, 2011–2012. Retrieved from https://mchb.hrsa.gov/nsch/2011-12/health/pdfs/nsch11.pdf