June 2019
|
June 2019 // Volume 57 // Number 3 // Research In Brief // v57-3rb4



Variables Affecting First-Time Parents' Feeding Behaviors
Abstract
After deciding whether to breastfeed or formula feed, parents must determine when to introduce solid foods. We examined feeding behaviors of 131 first-time parents, applying the theory of planned behavior to our investigation. Results indicated that parents' attitudes influenced infant feeding behavior at 6 months old. Therefore, Extension professionals should consider providing programming and materials to encourage healthful attitudes, in addition to focusing on general nutrition information. Moreover, our sample relied heavily on health professionals, friends and family, and books or videos for infant feeding information, so Extension professionals should consider targeting other influential groups in addition to targeting parents directly.
There is an abundance of research showing that parents' feeding practices can have long-term effects on infants' health, nutrition, and weight statuses (Haszard, Russell, Byrne, Taylor, & Campbell, 2019; Russell et al., 2018; Thompson, Adair, & Bentley, 2013). Infants who begin solid foods prior to 4 months are at an increased risk for choking, diabetes, allergies, food aversion, high blood pressure, and obesity (Avery & Baxter, 2001; Black, Siegel, Abel, & Bentley, 2001). Introducing solid foods after 6 months of age also may result in difficulties, including undernutrition, feeding problems, stress on the infant's digestive system, delayed growth and cognitive development, and increased risk of developing a wheat allergy (Hamilton, Daniels, White, Murray, & Walsh, 2011; Haszard et al., 2019; Horodynski et al., 2007).
The American Academy of Pediatrics (AAP) publishes recommendations for the introduction of solid foods, but early research on the topic showed that between 50% and 78% of infants were given solid foods earlier than recommended (Crocetti, Dudas, & Krugman, 2004). Parents who stray from recommendations cite various reasons for doing so, including the perspectives that doing so helps the infant sleep through the night or keeps the infant from spitting up (Horodynski et al., 2007; Scott, Binns, Graham, & Oddy, 2009) or that breast milk or formula alone is not enough to satisfy the infant (Horodynski & Mills, 2014).
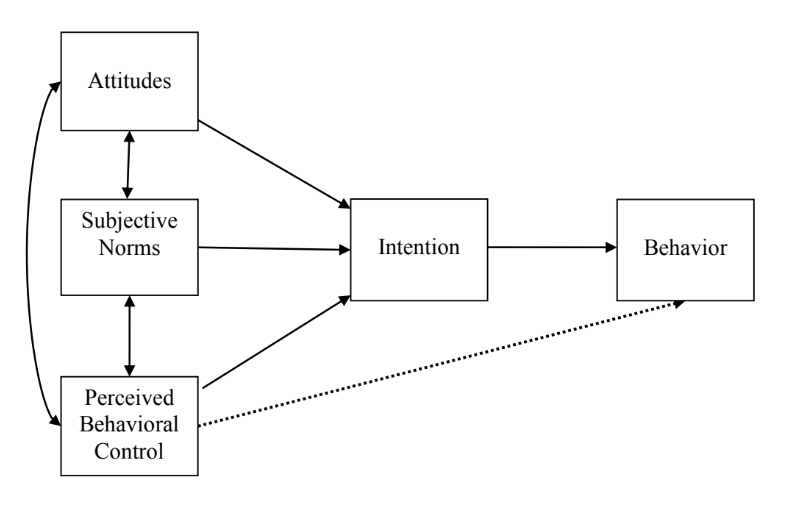
Although effects of parents' feeding practices on children's health have been studied often, most of the research has focused on preschool children rather than infants (Polfuss & Frenn, 2012), and few studies have addressed why parents decide to introduce solid foods when they do (Horodynski & Mills, 2014). To add to the literature, we conducted a study directed at addressing these gaps. We applied the theory of planned behavior (Ajzen, 1988) to identify variables that influence the timing of the introduction of solid foods. Originally applied to breastfeeding practices, the theory of planned behavior is a well-validated theoretical model that assumes that an individual's actions are based on his or her intent to perform, or not perform, a voluntary behavior. Behavioral intent is said to be determined by one's attitude toward the behavior, perceptions of relevant subjective norms, and perceived behavioral control. Furthermore, Ajzen (1988) believed that a person's stating intent to perform a certain behavior to someone else makes the person more likely to perform that behavior (see Figure 1 in the "Methods" section). Extension professionals may consider our findings when developing parent education programs and curricula.
Methods
Recruitment
We recruited participants to complete our online survey through social media, electronic mailing lists, and flyers that were distributed at child care centers, mothers' groups, and restaurants in the southeastern United States. Snowball sampling was encouraged. Participants had to give consent to participate in the study before beginning, were able to skip questions, could end the survey at any time, and had to confirm submitting their responses for their data to be used. Inclusion criteria for the study were that (a) the individual was a first-time parent, (b) the individual had only one child, and (c) the individual's child was an infant between 6 and 12 months old. Sample size was calculated at 120 (Norman & Streiner, 2003); after 1 month, the desired sample size was exceeded and so we proceeded with analyses.
Measures
Our survey addressed basic demographics; where the parent obtained information about breastfeeding, formula feeding, and introducing solid foods; and the age of the baby when the parent first gave the baby anything besides breast milk, formula, or water. As well, the survey included a variety of questions regarding the introduction of solid foods, including questions on why the parent chose to introduce solid foods, the age at which the parent had thought he or she would introduce solid foods before the baby was born, and the infant's feeding behaviors at 6 months old.
For the questions regarding the introduction of solid foods, we were guided by the literature on why parents introduce solid foods We constructed self-report items involving a 7-point scale ranging from strongly disagree to strongly agree. Items were organized by constructs in the theory of planned behavior (attitudes, subjective norms, perceived behavioral control, and intention) (Ajzen, 1991; Horodynski & Mills, 2014). We obtained measures for each construct by summing item responses. To establish content validity, four experts, all having doctoral degrees in human development and family science, analyzed all items. Additionally, to evaluate face validity, we pilot tested the measures with 11 parents who had children between 12 and 18 months of age.
To improve internal consistency, we conducted factor analysis on the items. Those that loaded poorly (<.5) were deleted because they did not appear to reliably assess the intended construct. Originally, the measures for all constructs comprised five items, except the measure for intention, which comprised four items. After factor analysis, the final measure for the attitudes construct comprised three items (α = .593); Hassad (2009) recommended a Cronbach's alpha of .6 or higher to establish an acceptable level of reliability, so .593 was deemed close enough to the acceptable limit. The final measure for subjective norms construct comprised five items (α = .709). The final measure for the perceived behavioral control construct comprised one item (α = .96); although one-item measures are not often used, studies have shown support for their use, especially in predicting future behavior (Hoeppner, Kelly, & Urbanoski, 2011). The final measure for the intention construct comprised four items (α = .656).
We assessed behavior using five items asking about the infant's feeding behaviors at 6 months old. Responses to the items were each coded as 0 = inappropriate or 1 = appropriate, according to current AAP feeding recommendations, and then summed to form a continuous index of the number of appropriate behaviors, ranging from 0 to 4 (0 = all behaviors were inappropriate, 4 = all behaviors were appropriate).
Statistical Methods
We calculated descriptive statistics, frequencies, and correlation analyses. Additionally, we obtained maximum likelihood estimates for the model we tested using path analysis (Figure 1). On the basis of the theory of planned behavior, we hypothesized pathways between attitudes, subjective norms, perceived behavioral control, intention, and behavior.
Figure 1.
Theory of Planned Behavior Model to Be Tested
Results
Sample
Our study included 131 first-time parents. Missing data were controlled through the use of discrete missing values. A majority of respondents identified themselves as the infant's mother (91.6%, f = 120). The sample predominantly identified as not Hispanic or Latino (95.4%, f = 125) and White (93.9%, f = 123). Parents' most commonly identified age group was 26 to 30 years (53.4%, f = 70). The majority held at least a bachelor's degree (45.8%, f = 60) or some type of postbaccalaureate degree (45.0%, f = 59). The sample also reported a high annual household income, with 71.3% (f = 92) reporting making $60,000 or more. Additionally, a majority of respondents were married to the infant's other parent (89.3%, f = 117).
Univariate Analyses
As noted, parents in our study were asked about their sources for obtaining information on breastfeeding, formula feeding, and introducing solid foods. One hundred percent of the sample reported obtaining information about breastfeeding from at least one source, 83.0% (f = 109) reported receiving information about formula feeding from at least one source, and 99.2% (f = 130) reported receiving information about introducing solid foods from at least one source. Most parents reported that a doctor, nurse, or other health professional had been the main source of the information about breastfeeding (92.4%, f = 121), formula feeding (68.8%, f = 75), and introducing solid foods (83.8%, f = 109) (Table 1). With regard to the number of sources for information on each topic, parents received information on breastfeeding from an average of 3.94 sources (SD = 1.37), information on formula feeding from an average of 2.51 sources (SD = 1.55), and information on feeding solid foods from an average of 2.95 sources (SD = 1.18).
| Source | Breastfeeding | Formula feeding | Feeding solid foods | |||
| f | % | f | % | f | % | |
| Doctor, nurse, or other health professional | 121 | 92.4% | 75 | 68.8% | 109 | 83.8% |
| WIC food program | 15 | 11.5% | 10 | 9.2% | 7 | 5.4% |
| Baby care class or support group | 87 | 66.4% | 33 | 30.3% | 20 | 15.4% |
| Relative or friend | 100 | 76.3% | 49 | 45% | 87 | 66.9% |
| Books or videos | 104 | 79.4% | 40 | 36.7% | 78 | 60% |
| Newsletters | 15 | 11.5% | 15 | 13.8% | 15 | 11.5% |
| Newspapers or magazines | 24 | 18.3% | 22 | 20.2% | 13 | 10% |
| Television or radio | 4 | 3.1% | 17 | 15.6% | 5 | 3.8% |
| Website | 50 | 38.2% | 13 | 11.9% | 49 | 37.7% |
| Note. WIC = Special Supplemental Nutrition Program for Women, Infants, and Children. | ||||||
We also asked the parent to identify the age at which the baby was first given anything besides breast milk, formula, or water. Over half of the sample (56.5%; f = 74) reported that the baby was 4 to 6 months when first given anything besides breast milk, formula, or water, and 36.6% (f = 48) reported that the baby was 6 to 8 months.
For each construct in the theory of planned behavior, we computed sum scores. For ease of interpretation of descriptive statistics, potential mean scores were computed, with possible ranges of 1–7. The mean score for parents' attitudes toward introducing solid foods was 3.01 (SD = 1.41), signifying low agreement with attitudes that often lead to early introduction of solid foods. Parents perceived the influence of subjective norms on their behavior to be low (M = 3.05, SD = 1.14), signifying that their feeding decisions were not perceived to be due to social influence/pressure. The mean score for the perceived behavioral control construct also was low (M = 3.02, SD = 1.92); parents had low agreement with the idea that they had introduced solid foods because the baby was unsatisfied. The mean score for intention was high (M = 5.23, SD = 1.26), indicating a high level of parental planning with regard to infant feeding. Finally, scores ranging from 0 to 4 were used to measure behavior signifying inappropriate feeding practices to appropriate feeding practices, respectively. On average, the parents in our sample were employing appropriate feeding practices when their babies turned 6 months old (M = 3.83, SD = 0.65). Table 2 shows frequencies of responses for the items comprising the five constructs.
| Item | Strongly disagree | Disagree | Somewhat disagree | Neither agree or disagree | Somewhat agree | Agree | Strongly agree | Yes | No |
| Attitudes | |||||||||
| I thought it would help my baby sleep longer at night | 53 | 27 | 2 | 12 | 22 | 12 | 3 | ||
| I felt my baby needed something in addition to breast milk or formula | 21 | 14 | 12 | 14 | 30 | 25 | 15 | ||
| I didn't think my baby weighed enough | 79 | 23 | 3 | 8 | 6 | 8 | 4 | ||
| Subjective norms | |||||||||
| A doctor or health professional said my baby should begin eating solid food | 39 | 6 | 3 | 21 | 18 | 51 | 20 | ||
| My baby's other parent said our baby should begin eating solid foods | 39 | 25 | 3 | 37 | 11 | 13 | 3 | ||
| Relatives said my baby should begin eating solid foods | 47 | 26 | 8 | 13 | 22 | 10 | 5 | ||
| Friends said my baby should begin eating solid foods | 49 | 31 | 11 | 19 | 13 | 6 | 2 | ||
| My employer said my baby should begin eating solid foods | 74 | 36 | 4 | 15 | 1 | 1 | 0 | ||
| Perceived behavioral control | |||||||||
| My baby seemed unsatisfied with breast milk/formula | 42 | 26 | 10 | 15 | 23 | 9 | 6 | ||
| Intentions | |||||||||
| I planned to feed my baby breast milk. . . | 2 | 2 | 4 | 1 | 6 | 24 | 92 | ||
| I knew what solid food I was going to introduce first | 9 | 18 | 9 | 6 | 45 | 22 | 22 | ||
| I knew how old I wanted my baby to be when I introduced him/her to solid food | 6 | 15 | 9 | 13 | 29 | 25 | 34 | ||
| My baby was introduced to solid food at the age I originally had planned | 22 | 6 | 4 | 3 | 23 | 40 | 33 | ||
| Behavior | |||||||||
| He/she was only drinking breast milk and/or formula and consuming no other foods or beverages | 58 | 73 | |||||||
| He/she was eating pureed solid food (homemade or store bought) | 73 | 58 | |||||||
| He/she was eating finger foods | 15 | 115 | |||||||
| He/she was drinking cow's milk, soy milk, or almond milk | 1 | 129 | |||||||
| He/she was eating the same foods I ate | 10 | 119 | |||||||
Correlation Analyses
Parents' attitudes were positively correlated with subjective norms, perceived behavioral control, and behavior (r = .35, .39, and .26, respectively; p < .01). Although two of the statistically significant correlations (attitudes and subjective norms and attitudes and perceived behavioral control) are consistent with the theory of planned behavior, the third statistically significant correlation (attitudes and behavior) suggested a pathway that was not included in the theoretical model.
Path Analyses
To test the theory of planned behavior, we conducted a path analysis to obtain maximum likelihood estimates. Overall, the model did not fit the data. However, as was found in the correlation analyses, attitudes and subjective norms and attitudes and perceived behavioral control were positively correlated with each other in the path analysis (β = .34, p < .01 and β = .39, p = <.01, respectively). Because the correlational analyses indicated a pathway that was not included in the theoretical model, we tested a second model (Figure 2) (Kenny, 2011).
Figure 2.
Results from Path Analysis with a Direct Link from Attitude to Behavior
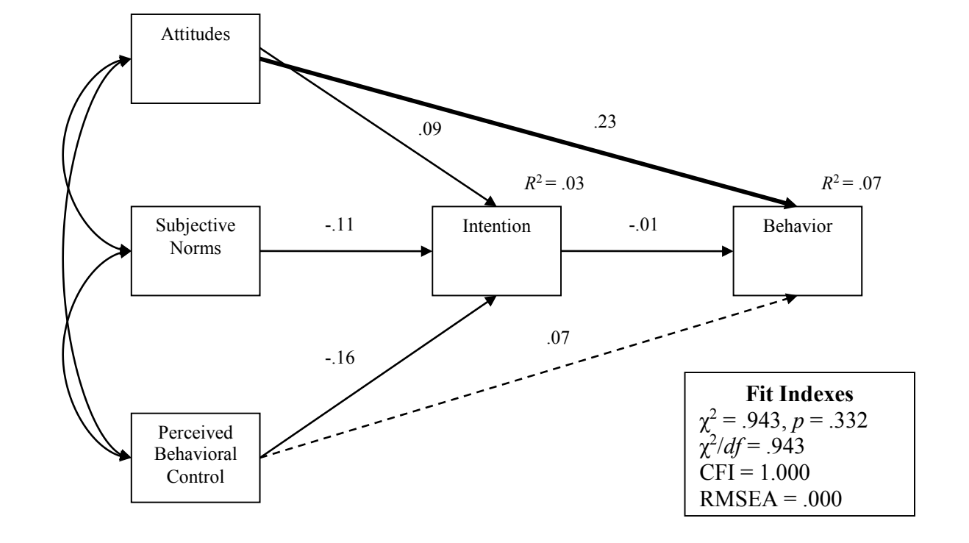
Note: CFI = comparative fit index. RMSEA = root mean square error of approximation.
The second model included a direct pathway from attitudes to behavior. There was a statistically significant association between attitudes and infant feeding behavior at 6 months old (β = .23, p < .01). The squared multiple correlations for intention and behavior were still small, at .03 and .07, respectively, although the coefficient for behavior increased slightly. All goodness-of-fit statistics were within acceptable ranges. Therefore, it appears that, overall, the second model fit the data.
Conclusion
The participants in our study relied heavily on health professionals, friends and family, and books or videos for infant feeding advice (Table 1). As a result, Extension professionals may want to broaden their educational reach. If they are educating a larger portion of the population, more people will be knowledgeable with regard to appropriate nutritional and feeding expectations for children, and thus individuals around new parents would be more likely to share valid information. To do this, Extension professionals may consider new, online methods of delivery as technological advances have made it easier to share health-related information electronically (Case, Cluskey, & Hino, 2011). Extension educators could create blogs, memes, infographics, and other easily shared items discussing appropriate nutrition and feeding transitions. They also could use social media platforms (i.e., Twitter) to broaden outreach on these topics.
Applying a modified theory of planned behavior, we found a statistically significant direct path from attitudes to behavior. Extension professionals should consider this path when developing and administering parenting/nutrition education curricula, focusing on encouraging healthful attitudes, not just on increasing general knowledge. Moreover, because educational/knowledge-building approaches are not always successful in changing attitudes and the attitudes we measured (Table 2) are often deeply rooted in culture and generational beliefs, Extension professionals should consider developing parent education curricula and materials that involve the entire family, thereby increasing the chances that feeding decisions will be based on healthful attitudes (Horodynski & Mills, 2014). Extension professionals also may consider conducting guest lectures in family and consumer science classes in high schools to reach younger generations before they become parents.
Participants in our study were mostly Caucasian, older (for first-time parents), married, and highly educated with reported high annual incomes. This sample is not representative of the population as a whole, so results may not be generalizable to a larger population. Future research should involve a more diverse sample. Dyadic data also would provide great insight into how parents influence each other in their feeding decisions. Our study assumed AAP recommendations; however, responses could differ if parents follow different feeding recommendations (i.e., recommendations from the Special Supplemental Nutrition Program for Women, Infants, and Children). To account for this scenario, future studies should involve asking parents what recommendations they follow, what conflicting information they have received with regard to the introduction of solid foods, and what they do when they encounter conflicting information.
References
Ajzen, I. (1988). Attitudes, personality and behavior. Chicago, IL: Dorsey Press.
Ajzen, I. (1991). The theory of planned behavior. Organizational Behavior and Human Decision Processes, 50, 179–211.
Avery, A., & Baxter, A. (2001). "Change to cup": An audit to determine parental awareness and practices in changing from bottle to cup. Journal of Human Nutrition and Dietetics, 14, 217–223.
Black, M. M., Siegel, E. H., Abel, Y., & Bentley, M. E. (2001). Home and videotape intervention delays early feeding solid food among adolescent mothers. Pediatrics, 107(5), 1–8. doi:10.1542/peds/107.5.e67
Case, P., Cluskey, M., & Hino, J. (2011). Online nutrition education: Enhancing opportunities for limited-resource learners. Journal of Extension, 49(6), Article 6RIB5. Available at: https://www.joe.org/joe/2011december/rb5.php
Crocetti, M., Dudas, R., & Krugman, S. (2004). Parental beliefs and practices regarding early introduction of solid foods to their children. Clinical Pediatrics, 43(6), 541–547.
Hamilton, K., Daniels, L., White, K. M., Murray, N., & Walsh, A. (2011). Predicting mothers' decisions to introduce feeding solid food at 6 months. An investigation using an extended theory of planned behaviour. Appetite, 56, 674–681. doi:10.1016/j.appet.2011.02.002
Hassad, R. (2009). Development and validation of a teaching practice scale (TISS) for instructors of introductory statistics at the college level. Hague, Netherlands: International Association for Statistical Education—International Statistical Institute. Retrieved from http://arxiv.org/ftp/arxiv/papers/1007/1007.3654.pdf
Haszard, J. J., Russell, C. G., Byrne, R. A., Taylor, R. W., & Campbell, K. J. (2019). Early maternal feeding practices: Associations with overweight later in childhood. Appetite, 132, 91–96.
Hoeppner, B. B., Kelly, J. F., & Urbanoski, K. A. (2011). Comparative utility of single-item vs. multiple-item measure of self-efficacy in predicting relapse among young adults. Journal of Substance Abuse Treatment, 41(3), 305–312. doi:10.1016/j.jsat.2011.04.005
Horodynski, M. A., & Mills, K. J. (2014). The voice of low-income adolescent mothers on infant feeding. Journal of Extension, 52(6), Article 6RIB5. Available at: https://www.joe.org/joe/2014december/rb5.php
Horodynski, M., Olson, B., Arndt, M. J., Brophy-Herb, H., Shirer, K., & Shemanski, R. (2007). Low-income mothers' decisions regarding when and why to introduce solid foods to their infants: Influencing factors. Journal of Community Health Nursing, 24(2), 101–118.
Kenny, D. A. (2011). Respecification of latent variable models. Retrieved from http://davidakenny.net/cm/respec.htm
Norman, G. R., & Streiner, D. L. (2003). Path analysis and structural equation modeling. In PDQ Statistics (pp. 156–176). Retrieved from http://fhs.mcmaster.ca/surgery/documents/pdq_stats.pdf
Polfuss, M. L., & Frenn, M. (2012). Parenting and feeding behaviors associated with school-aged African American and White children. Western Journal of Nursing Research, 34(5), 677–696. doi:10.1177/0193945911402225
Russell, C. G., Haszard, J. J., Taylor, R. W., Heath, A. M., Taylor, B., & Campbell, K. J. (2018). Parental feeding practices associated with children's eating and weight: What are parents of toddlers and preschool children doing? Appetite, 128, 120–128. doi:10.1016/j.appet.2018.05.145
Scott, J. A., Binns, C. W., Graham, K. I., & Oddy, W. H. (2009). Predictors of the early introduction of solid foods in infants: Results of a cohort study. BCM Pediatrics, 9, 60. doi:10.1186/1471-2431-9-60.
Thompson, A. L., Adair, L. S., & Bentley, M. E. (2013). Pressuring and restrictive feeding styles influence infant feeding and size among a low-income African-American sample. Obesity, 21(3), 562–571. doi:10.1002/oby.20091