April 2018
|
April 2018 // Volume 56 // Number 2 // Ideas at Work // v56-2iw1



Extension: The Backbone Organization in Statewide Population Health Management
Abstract
Clemson University Cooperative Extension Service has developed and is implementing a statewide population health management model aimed at leveraging key partnerships in South Carolina. The model delineates roles of key partners needed to operationalize statewide initiatives and drive the delivery of health extension in the state. Clemson University Cooperative Extension functions as the backbone organization within the model, achieving collective impact by using a collaborative approach for cultivating health as a shared value of entities throughout the state. Strong partnerships have been established, and rigorous evaluation is under way to determine the model's efficacy with regard to health indicators and population health outcomes.
Introduction
An individual's health status is heavily determined by factors other than health care. Lifestyle, genetics, socioeconomic factors, access to community resources, and the physical environment play significant roles, especially as health trends increasingly shift from infectious and acute diseases to chronic conditions. New approaches that coordinate resources and aid community members in navigating health systems are needed to foster a culture of health (Robert Wood Johnson Foundation, 2016) in the places where people live, work, learn, and play. Land-grant universities, such as Clemson University (CU), have the community presence, local credibility, and partnership networks to effectively coordinate health resources, influencing the social, economic, and environmental determinants of health (Braun et al., 2014). CU Cooperative Extension Service has developed a statewide population health management delivery model that not only leverages partnerships but does so with Extension at the center, serving as the backbone organization for collective impact.
South Carolina's health ranking in 2015, compared with all other states, was 42 (United Health Foundation, 2015). Two factors contributing to poor health outcomes in South Carolina are the large number of rural communities and their associated poverty (Wong & Regan, 2009). Over half of the state's 46 counties are at least 50% rural (University of Wisconsin Population Health Institute, 2016), a designation associated with limited access to primary health care providers due to supply and distance (Rural Health Foundation, 2016). Thirty-four counties in South Carolina are designated as primary care health professional shortage areas (Health Resources and Services Administration, 2016). In one rural county in South Carolina, this designation equates to a ratio of one primary care provider to every 9,000 residents.
Poverty is a persistent issue in rural counties (Andress & Fitch, 2016), and in South Carolina, rural communities have high rates of unemployment, children living in poverty, and food insecurity (University of Wisconsin Population Health Institute, 2016). Resulting health outcomes include higher than national and state averages for premature death, poor overall health status, and high rates of obesity, physical inactivity, and chronic health conditions (University of Wisconsin Population Health Institute, 2016). These significant health disparities suggest that the conventional ways of accessing traditional health care delivery systems are inadequate.
Cooperative Extension is well positioned to address this problem. The Health Task Force of the Extension Committee on Organization and Policy identified eight core themes that serve as guiding principles for strengthening Extension's impact on the health outcomes of Americans (Braun et al., 2014). Building partnerships and acquiring resources, within the university and community-based organizations, is one core theme. Although it is clear that a creative, collaborative, and comprehensive approach for improving health outcomes is needed, aligning partners to pursue a common agenda for any length of time raises a new set of leadership challenges.
Kania and Kramer (2013) identified the need for strong leadership in the form of a backbone organization, functioning to pull partners together and keep them moving in the direction of a shared strategic plan. Extension agents are experts at facilitating two-way communication and find their roots in serving as community "organizers" (Peters, 2002). This organizing lends itself to leadership as partners are challenged to identify who will coordinate and build consensus. Therefore, Extension is the ideal backbone organization for collective impact in statewide health program delivery.
Kania and Kramer (2013) described six essential functions to be performed by a coordinating organization pursuing collective impact with its partners. These functions are
- facilitating dialogue among partners,
- providing overall strategic direction,
- coordinating community outreach,
- managing data collection and analysis,
- handling communications, and
- mobilizing funding.
This article describes a statewide population health delivery model that leverages partnerships, with Extension serving in the central communication role and functioning as the backbone organization for collective impact in the state.
Approach
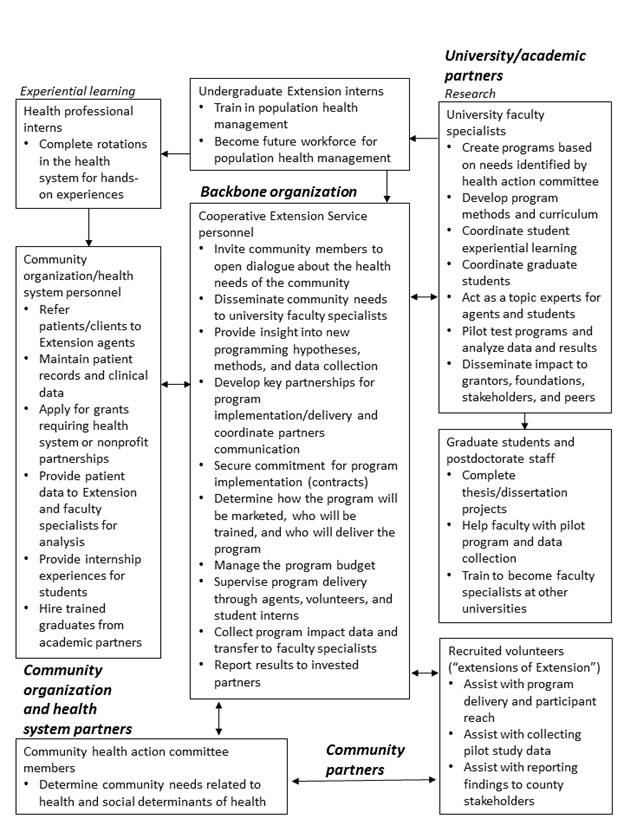
The South Carolina statewide population health delivery model (Figure 1) has four key points for action: (a) community, (b) CU Cooperative Extension, (c) university/academic partner, and (d) community organization or health system partner.
- The model begins with Point 1, the community, where needs related to health access, health education, and social determinants of health are identified.
- Point 2 is Extension, which focuses on leveraging existing partnerships and creating new partnerships with academic units, community organizations, and health systems to problem solve around community health needs. As the backbone organization, Extension serves as the communication hub, facilitating communication among community members, academicians, and community health service/health system organizations. Table 1 highlights the ways in which South Carolina's Extension agents fulfill the functions of a backbone organization.
- Point 3 is the university/academic partner, which coordinates curriculum and student training experiences with Extension and health system partners. Faculty specialists develop and pilot test community health programs through Extension, ultimately transferring evidence-based health programs to communities.
- The community organization or health system partner is Point 4 in the model. Community organizations include the Department of Education, the Department of Health and Environmental Control, free health clinics, and food pantries or food banks. These organizations can provide referrals, physical locations for program implementation, and financial support for program delivery. The health system provides similar support to the program but also provides access to data from patient medical records and other sources for use in evaluating program impact and outcomes. Additionally, the health system provides experiential learning for nursing, public health, and allied health professionals and serves as an employment pipeline for university nursing and public health science graduates.
Figure 1.
Statewide Population Health Management Model and Partner Role Delineation
| Function | CES fulfillment of the function |
| Function 1: Facilitating dialogue among partners | CES agents create and coordinate community health action committees in counties or regions. The agents relay community needs to university faculty specialists in health, nutrition, agriculture, or food science departments. CES agents communicate needs and program development progress to health system and community organization partners. |
| Function 2: Providing overall strategic direction | As cogs in the communication hub, CES agents know what services are already in the community and where gaps exist. This role places the CES agent in a prime position for strategic planning and coordinating of health resources to reach a common end goal for the community. |
| Function 3: Coordinating community outreach | A well-known characteristic of Extension agents is their ability to understand and embed themselves within the communities they serve. CES agents' own experiences and community relationships give them valuable insight on how best to implement new programs and services without duplicating efforts. |
| Function 4: Managing data collection and analysis | CES agents collect pre- and postprogram knowledge and behavior scores for all programs delivered and have experience gathering important impact data to demonstrate efficacy of programming. Health systems can be a resource for important objective data, gathered from participant medical records (blood pressure figures, blood glucose values, number of hospital admissions, admission diagnoses, and discharge plans). The CES agent collects all data and transfers the data to faculty specialists who analyze the data and interpret results. |
| Function 5: Handling communications | CES agents not only handle partner communications in coordinating health care efforts but also disseminate information and results to stakeholders, community members, and partners through Extension fact sheets, journal publications, and professional and stakeholder presentations. |
| Function 6: Mobilizing funding | CES agents use statewide partnerships to establish contracts and memoranda of understanding where programming will be implemented. A business model is used in these contracts where fees for services are charged. Results of program evaluation spawn further financial support through faculty specialists' grants and community organization and health system contracts. |
| Note. CES = Clemson University Cooperative Extension Service. | |
Putting It into Practice
The population health management model presented here demonstrates a process for implementing a statewide population health initiative and is being tested in South Carolina. Rigorous evaluation of the model is under way to determine the model's efficacy with regard to health indicators and population health outcomes. Collaborative partnerships are essential, and CU Cooperative Extension serves as the communication hub and backbone organization for facilitating those relationships. The model delineates roles of key partners to operationalize statewide initiatives and drives the delivery of statewide health extension in South Carolina.
References
Andress, L., & Fitch, C. (2016). Rural health inequities and the role of Cooperative Extension. Journal of Extension, 54(3), Article 3FEA4. Available at: https://www.joe.org/joe/2016june/a4.php
Braun, B., Bruns, K., Kronk, L., Fox, L. K., Kukel, S., Le Menestrel, S., . . . Warren, T. (2014). Cooperative Extension's national framework for health and wellness. Issue brief. Retrieved from http://www.aplu.org/members/commissions/food-environment-and-renewable-resources/CFERR_Library/national-framework-for-health-and-wellness/file?id=5134
Health Resources and Services Administration. (2016). HPSA Find. Retrieved from http://datawarehouse.hrsa.gov/tools/analyzers/HpsaFind.aspx
Kania, J., & Kramer, M. (2013). Embracing emergence: How collective impact addresses complexity. Retrieved from https://ssir.org/articles/entry/embracing_emergence_how_collective_impact_addresses_complexity
Peters, S. (2002). Rousing the people on the land: The roots of the educational organizing tradition in Extension work. Journal of Extension, 40(3), Article 3FEA1. Available at: http://www.joe.org/joe/2002june/a1.html
Robert Wood Johnson Foundation. (2016). From vision to action: A framework and measures to mobilize a culture of health. Retrieved from http://www.rwjf.org/content/dam/COH/RWJ000_COH-Update_CoH_Report_1b.pdf
Rural Health Foundation. (2016). What's different about rural health care. Retrieved from http://www.ruralhealthweb.org/go/left/about-rural-health/what-s-different-about-rural-health-care
United Health Foundation. (2015). America's health rankings, 2015 annual report: Explore health measures in South Carolina. Retrieved from http://www.americashealthrankings.org/explore/2015-annual-report/measure/Overall/state/SC
University of Wisconsin Population Health Institute. (2016). County health rankings & road maps: South Carolina. Retrieved from http://www.countyhealthrankings.org/app/
Wong, S., & Regan, S. (2009). Patient perspectives on primary health care in rural communities: Effects of geography on access, continuity and efficiency. Rural and Remote Health, 9(1142). Retrieved from http://www.rrh.org.au/publishedarticles/article_print_1142.pdf