June 2016
|
June 2016 // Volume 54 // Number 3 // Feature // v54-3a4



Rural Health Inequities and the Role of Cooperative Extension
Abstract
Health inequities affect communities through adverse health outcomes, lost productivity, and increased health care costs. They arise from unequal distribution of social determinants of health—the conditions in which people are born and live. Health outcomes, tied to behaviors and health care, also are rooted in location and social status. Cooperative Extension provides culturally appropriate programs that touch the places where individuals and families live. A history of promoting democracy through education makes Extension uniquely positioned to address health inequities and foster greater equality among groups that experience hardships as a result of differences in social, economic, and environmental determinants of health.
Introduction
Health inequities, which are systematic differences in the health statuses of population groups, affect communities through adverse health outcomes, lost productivity, and increased health care costs. Health inequities grow out of the unequal distribution of the social determinants of health (SDOH)—the conditions in which people are born, grow, live, work, and age.
Since its creation, the Cooperative Extension System has provided culturally appropriate programs and services that touch the places where individuals and families work, live, and play. Because of its interest in creating a democratic society through the provision of education to all groups (Kelsey, 2002), Extension is uniquely designed to address health inequities in rural areas (Association of Public and Land-Grant Universities, 2012) and to foster greater equality among groups that experience hardship as a result of differences in SDOH. The objectives of this article are to define health inequities and to discuss the role of Extension and the land-grant university in helping eliminate them.
Health Inequities and SDOH
The World Health Organization (WHO) Commission on the Social Determinants of Health presented two definitions of SDOH:
- The circumstances in which people are born, grow up, live, work, and age and the systems put in place to deal with illness. These circumstances are in turn shaped by a wider set of forces—economics, social policies, and politics (World Health Organization [WHO] Commission on Social Determinants of Health, 2013).
- The complex, integrated, and overlapping social structures and economic systems that are responsible for most health inequities. These social structures and economic systems include the social environment, the physical environment, health services, and structural and societal factors (WHO Commission on Social Determinants of Health, 2015).
The concept of SDOH might be characterized as public health's effort to integrate a model of health production chiefly constructed around individual behavior within a larger framework of factors that establish the society in which we live. In this model, health outcomes are created by a combination of personal behavior and an overlay of external factors that are beyond the control of the individual and in the hands of institutions, systems, and decision makers who craft policies, rules, and regulations.
The SDOH model offers a second opportunity for an expansive model of public health, one that resembles the agenda of the early 20th century, when social conditions were integrated into the array of factors that shaped health. Within an SDOH framework, health promotion efforts involve a broader scope of responsibility that includes social conditions and related policies and issues. Summarily, an SDOH framework means that health outcomes, in addition to being tied to behaviors and health care, are also rooted in location and social status.
The incidence of type 2 diabetes mellitus (T2DM) in the United States offers an example for exploring the relationship between health inequities and socioeconomic status. In the United States, the healthiest counties have better high school graduation rates and college attendance, whereas the least healthy counties have higher unemployment, more children living in poverty, higher violent crime rates, more deaths due to injuries, and more people without sufficient social support (University of Wisconsin Population Health Institute, 2014). The poor, living in areas where poverty is prevalent and pervasive, face impediments beyond those of their individual circumstances. Concentrated, long-term poverty contributes to poor housing, low graduation rates, poor health conditions, higher crime rates, and employment dislocations. As a result, economic conditions in very poor areas create a lack of opportunities that becomes deeply entrenched and self-perpetuating (U.S. Department of Agriculture Economic Research Service, 2014). T2DM is an example of a health issue that disproportionately affects low-income groups. The prevalence of T2DM is highest in counties with high rates of poverty and unemployment and limited access to health-producing community amenities.
Because the highest rates of deep poverty are clustered in rural areas (Farrigan, Hertz, & Parker, 2014), an important issue for rural areas is the link between poverty and T2DM. An analysis of poverty rates and obesity across 3,139 counties in the United States found that people who live in the most poverty-dense counties are more prone to obesity and diabetes (Levine, 2011). The profile of those states that are rural and have high levels of poverty demonstrates large differences in rates of T2DM by groups disaggregated by gender, age, race, geography, and socioeconomic status (Grintsova, Maier, & Mielck, 2014). Socioeconomic status may affect the incidence of T2DM directly and indirectly relative to access to and quality of health care, social support, community resources, diabetes education, treatment choices, and recommended medication. Thus, low socioeconomic status and residence in a rural area could be associated with multiple risks (Connolly, Unwin, Sherriff, Bilous, & Kelly, 2000).
Most of the county-to-county variance in obesity can be accounted for by variance in sedentariness, which may be explained by limited county revenues to pay for infrastructure, including sidewalks, parks, biking/walking trails, and subsidized sport facilities (Levine, 2011). Further, having little or no income hinders the ability of families to pay for, or local governments to subsidize, gym memberships, participation in sports activities for children, and sports/exercise clothing or equipment. Even simply the state of being a rural area—compared to being an urban, nonfarm area—contributes to inequities in rates of T2DM. Although most food access policy research focuses on urban communities, residents of rural communities face a disproportionately higher risk for nutrition-related chronic diseases (Johnson et al., 2014).
Rural areas differ from one another, of course, but similarities across such areas provide a picture of the general inequities in rural areas:
- Rural residents generally consume fewer fruits and vegetables than urban or suburban residents do.
- Obesity prevalence is 39.6% among rural adults, compared to 33.4% among urban adults, and remains significantly higher after controlling for demographics, diet, and physical activity.
- Children living in rural communities versus urban communities are more likely to be overweight or obese.
A Framework for Action on Health Inequities Relative to Diabetes, Using SDOH
To consider how Extension's programs and activities incorporate SDOH to address health inequities, we will continue to use diabetes as an example and apply two principles and an overarching strategy.
Principle 1: A comprehensive approach to reducing inequities relative to diabetes involves a combination of policies that address inequities in root SDOH and policies that treat the symptoms or compensate for inequities in SDOH. Community-based, multicomponent interventions that address both individual-level factors and social determinants have been proved successful in improving diets and increasing physical activity levels among those living in deprived areas. Successful interventions have focused on a range of determinants, including capacity building, community participation, community development, systems change, health education, food preparation, and physical activity classes. For example, in addition to using short-term strategies to improve individual knowledge and behaviors among low-income groups, policies to address contextual factors are needed. High-priority policies and structural changes would increase access to physical activity by using a sliding-fee scale for fitness centers; would reduce or restrict food advertising to children; would make healthful food less expensive; would put in place macrolevel policies having long-term focuses of reducing poverty (such as minimum wage and social benefits); would promote resilience (such as by teaching life skills at school); and would reduce social exclusion through community participation (Brunner, Cohen, & Toon, 2001).
Principle 2: Once it is known which groups experience the highest rates of diabetes, care must be taken to ensure that a program, a policy, or an activity works for the groups experiencing the inequities or most in need. If diabetes is more prevalent in socially disadvantaged groups yet policies and interventions are more effective in advantaged groups, the use of those policies and interventions with all groups increases the likelihood that inequities in the rate of diabetes among groups will widen, lessening chances of reducing overall prevalence (Loring & Robertson, 2014). For example, education campaigns on obesity without structural support (subsidies to help pay the high cost of interventions for low-income groups) may widen inequities. Low-income groups are less able to act on new information—lack of money and lack of affordability, accessibility, and availability of foods create barriers that often are the deciding factors when purchasing food. Information alone will not be effective without measures to enhance the ability of poor and marginalized groups to act on this information. Moreover, where information dissemination strategies are used, specific effort is needed to ensure that the messages are designed with and for the most disadvantaged groups. For example, consumers with low numeracy or literacy skills may be more receptive to pictograms/pictures or labeling.
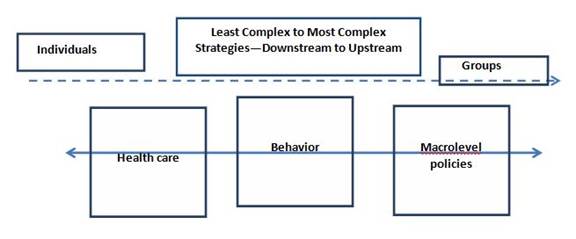
Strategy: The overarching strategy involves an "equity action spectrum" that integrates a mix of simple and complex interventions ranging in nature from approaches with individuals to approaches that begin to address population health (WHO Regional Office for Europe, 2014). One way to think about an equity action spectrum is to understand that action lies along a continuum, moving from the least complex and impactful efforts to reduce inequities toward more intricate endeavors involving systems or policy change (Figure 1). Implementation of these complicated efforts is sometimes referred to as going "upstream" to address the "causes of the causes" to prevent inequities (WHO Regional Office for Europe, University College of London Institute of Health Equity, 2013). Health care is farthest to the left because it (a) is least impactful (i.e., helps one person at a time, not populations) and (b) is introduced after a person or groups are already ill. Figure 1 shows that because behavior change is closer to a prevention strategy, it lies farther along the continuum than health care. However, behavior change is strained as an effective equity strategy because it is harder for low-income populations to be successful at behavior change while confronting social issues that limit their choices and abilities. Accordingly, the most complex efforts—including policy, systems, and social changes (e.g., housing, transportation, employment, governance, and economic policies)—lie farthest to the right, or upstream, on the continuum. These are SDOH that affect large numbers of people on the basis of their social statuses.
Figure 1.
Equity Action Spectrum
Extension Services and the Equity Action Spectrum
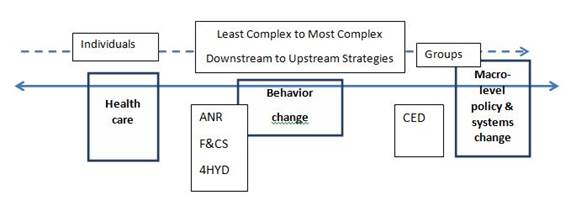
As Figure 2 shows, the major program areas of Extension—agriculture and natural resources (ANR), family and consumer sciences (F&CS), 4-H youth development (4HYD), and community and economic development (CED)—can be placed on the equity action spectrum. The positions of the major program areas on the spectrum are based on two factors:
- impact (e.g., individuals versus groups) and
- complexity (e.g., behavior change versus social change).
Figure 2.
Equity Action Spectrum and Extension Program Areas
Extension Programs and Downstream Efforts
Low-income groups typically reside in areas with a denser supply of fast food outlets, less availability of fresh vegetables and fruits, and unsafe, unkempt, or nonexistent spaces for physical activity. Further, low socioeconomic groups may experience chaotic living conditions, with day-to-day cash flow problems, making planning, budgeting, storing, and preparing healthful meals difficult (Robertson, Lobstein, & Knal, 2007). These limited community resources and daily chaotic conditions mean that low-income groups have increased exposure to the determinants of diabetes due to the food and physical activity environments in which they live and work, including differential exposure to positive and negative influences. Extension offers programs across three of its four major program areas that address individual health care decisions and behavior change. Extension programs in ANR, F&CS, and 4HYD work downstream, using educational and behavioral strategies with individuals. ANR, F&CS, and 4HYD programs contribute to efforts to improve SDOH by protecting vulnerable groups from differential exposure to food access and physical activity:
- ANR programs teach people to raise their own food. They also enhance access to healthful foods through farm-to-school programs or local farmers' markets.
- F&CS programs emphasize the individual and vulnerabilities in behavior that put individuals at greater risk for health problems. F&CS programming provides financial resource management education; general nutrition, health, and wellness classes; food safety and food preservation classes; and diabetes prevention and self-management support. Multistate programs, such as Strong Women and Dining with Diabetes, provide instruction and support for lifestyle changes that reduce risk and promote well-being. Health care and health literacy programs increase the capacity of participants to make informed decisions about health care and insurance. Educators with the Expanded Food and Nutrition Education Program help low-income adults with young children develop knowledge and skills in meal planning and preparation, food safety, and food resource management.
- 4HYD programs also emphasize the individual and vulnerabilities in behavior. Vulnerabilities that contribute to inequities in diabetes can be social (e.g., low self-esteem can cause members of disadvantaged groups to devalue their ability to be successful) or biological (e.g., infants born, with high or low birth weight, to an obese mother are more likely to develop obesity and/or diabetes later in life) (Levine, 2011). Examples of programming may include interventions that (a) pay special attention to overweight groups, taking into account that self-esteem tends to be lower among individuals in such groups, and (b) reduce the social isolation of low-income individuals and ensure that programs (job training, education, or sports services) do not favor people with high educational achievements or elite abilities (Robertson et al., 2007). 4HYD programs address vulnerabilities in behavior that could contribute to diabetes by providing young people with skills and resources targeting or preventing such vulnerabilities, including programs promoting healthful lifestyles (e.g., tobacco prevention, antibullying, personal development, and obesity prevention programs); civic and global engagement; and academic achievement and college preparation.
Extension Programs and Upstream Efforts
Upstream efforts focus on systems change as opposed to individual behaviors. Extension programs in CED approach the far end of the spectrum, among the more complex, upstream efforts, because they protect vulnerable groups in rural areas on the basis of economic conditions. SDOH are related to socioeconomic contexts. For example, socioeconomic contexts can affect the distribution of SDOH through factors that influence how food is produced, distributed, and consumed, determining which groups are most at risk of diabetes. These factors may be modifiable by raising incomes of the poorest groups through social protection, minimum wages, and redistributive taxation and by ensuring that assistance programs include healthful food, thereby reducing health inequities (Brunner et al., 2001). CED programs provide workforce education and leadership training for elected and appointed community leaders, with a goal of facilitating policy and systems change. CED programs support community development endeavors, including economic impact assessments, community planning for walkability and other transportation issues, sustainable food systems that increase food access, business retention and expansion for job growth and economic development, and tourism studies that can increase jobs, wages, and exposure to physical activities.
Conclusion and Call to Action
Extension has many programs that address health inequities by using an SDOH framework. Further, Extension's National Framework for Health and Wellness (National Framework), approved in March 2014, features six priorities that array themselves along the equity action spectrum. Priorities that are individual-based educational efforts and fall on the left of the spectrum are health literacy, chronic disease prevention and management, health insurance literacy, and positive youth development. Priorities that are more oriented toward system change and fall on the right of the spectrum are integrated nutrition, health, environment, and agriculture systems and health policy issues education (Rodgers & Braun, 2015).
Consistent with the equity action spectrum described herein, Extension programs and the priorities of the National Framework integrate action across the health equity continuum by including both individual-based efforts and systems initiatives that tackle SDOH. However, other issues exist that Extension should consider and address in the future. Recall that Principle 2 advises that care must be taken to ensure that a program, a policy, or an activity is tailored to the groups most in need. In essence, the idea is that one-size-fits-all policies and programs do not work. In this case, once it is known that certain groups have higher rates of disease according to social status, policies or programs must be tailored to those groups. It is difficult to determine which of the programs used by Extension target disadvantaged populations. Further, it is not clear whether the strategies that might work well for a general population have been examined for their efficacy with vulnerable groups.
Extension began in the early 20th century, at a time when public health practice focused on sanitation, social conditions, housing, poverty, and other external factors that shaped a community's behavior. By incorporating an SDOH model into relevant goals and programming, we have a second opportunity in the United States for an expansive model of public health that is closer to the agenda of the early 20th century, when social conditions were integrated into the array of factors that shaped health. With both Extension and public health using an SDOH framework, it is conceivable for efforts that address population health problems to bear a broader scope of responsibility that includes not just the individual and the body but also social conditions and related policies and issues.
References
Association of Public and Land-Grant Universities. (2012). The Land Grant Tradition. Washington, D.C.: Author. Retrieved from http://www.aplu.org/page.aspx?pid=1593
Brunner, E., Cohen, D., & Toon, L. (2001). Cost effectiveness of cardiovascular disease prevention strategies: A perspective on EU food based dietary guidelines. Public Health Nutrition, 4, 711–715.
Connolly, V., Unwin, N., Sherriff, P., Bilous, R., & Kelly, W. (2000). Diabetes prevalence and socioeconomic status: A population based study showing increased prevalence of type 2 diabetes mellitus in deprived areas. Journal of Epidemiology and Community Health, 12, 173–177.
Farrigan, T., Hertz, T., & Parker, T. U.S. Department of Agriculture, Economic Research Service. (March 2014). Retrieved from http://www.ers.usda.gov/amber-waves/2014-march/poverty-and-deep-poverty-increasing-in-rural-america.aspx#.VKFswcAw
Grintsova, O., Maier, W., & Mielck, A. (2014). Inequalities in health care among patients with type 2 diabetes by individual socio-economic status (SES) and regional deprivation: A systematic literature review. International Journal for Equity in Health, 13(43). doi:10.1186/1475-9276-13-43
Johnson, D. B., Quinn, E., Sitaker, M., Ammerman, A., Byker, C., Dean, W., . . . Sharkey, J. (2014). Developing an agenda for research about policies to improve access to healthy foods in rural communities: A concept mapping study. BMC Public Health, 14, 529. doi:10.1186/1471-2458-14-529.
Kelsey, K. D. (2002). What is old is new again: Cooperative Extension's role in democracy building through civic engagement. Journal of Extension [online], 40(4) Article 4COM1. Available at: http://www.joe.org/joe/2002august/comm1.php
Levine, J. (2011). Poverty and obesity in the U.S. Diabetes, 60, 2667–2668.
Loring, B., & Robertson, A. (2014). Obesity and inequities: Guidance for addressing inequities in overweight and obesity. World Health Organization. Retrieved from http://www.euro.who.int/__data/assets/pdf_file/0003/247638/obesity-090514.pdf?ua=1
Robertson, A., Lobstein, T., & Knal, C. (2007). Obesity and socio-economic groups in Europe: Evidence review and implications for actions. Brussels, Belgium: European Commission. Retrieved from http://ec.europa.eu/health/ph_determinants/life_style/nutrition/documents/ev20081028_rep_en.pdf
Rodgers, M., & Braun, B. (2015). Strategic directions for Extension health and wellness programs. Journal of Extension [online], 53(3) Article 3TOT1. Available at: http://www.joe.org/joe/2015june/tt1.php
University of Wisconsin Population Health Institute. County Health Rankings Key Findings. (2014). Retrieved from http://www.countyhealthrankings.org/sites/default/files/2014%20County%20Health%20Rankings%20Key%20Findings.pdf
U.S. Department of Agriculture, Economic Research Service. Geography of Poverty. (July 2014). Retrieved from http://www.ers.usda.gov/topics/rural-economy-population/rural-poverty-well-being/geography-of-poverty.aspx
World Health Organization (WHO) Commission on Social Determinants of Health. (May 7, 2013). Retrieved from http://www.who.int/social_determinants/sdh_definition/en/
WHO Commission on Social Determinants of Health. Social Determinants of Health, Key Concepts. (2015). Retrieved from http://www.who.int/social_determinants/thecommission/finalreport/key_concepts/en/
WHO Regional Office for Europe. New evidence-based tools to reduce health inequities in Europe. Fact sheet. Copenhagen. (June 16, 2014). Retrieved from http://www.euro.who.int/__data/assets/pdf_file/0019/252118/Fact-sheet-Evidenced-based-tools-vs-health-inequity.pdf?ua=1
WHO Regional Office for Europe, University College of London Institute of Health Equity. Review of the social determinants and the health divide in the WHO European Region: Executive Summary. (2013). Retrieved from http://www.instituteofhealthequity.org/projects/who-european-review