December 2014
|
December 2014 // Volume 52 // Number 6 // Research In Brief // v52-6rb5



The Voice of Low-Income Adolescent Mothers on Infant Feeding
Abstract
Adolescent mothers' feeding practices impact infant weight gain. Infant obesity, especially in low-income families, is rapidly increasing. The aim of the exploratory study reported here was to identify factors affecting low-income African American and non-Hispanic White adolescent mothers' infant feeding practices and useful learning modalities. Two focus groups were conducted by a trained facilitator using a semi-structured topic guide. Three themes emerged: (1) feeding decisions related to introduction of solid foods; (2) feeding information/advice provided by others; and (3) useful learning strategies. These themes can be used by Extension professionals in designing nutrition education programs for adolescent mothers.
Introduction
Excessive weight gain in infancy is closely linked with feeding practices (Mihrshahi, Battistutta, Magarey, & Daniels, 2011). Low-income, adolescent, first-time mothers are less likely to engage in infant feeding associated with healthy growth, which is crucial in reducing childhood obesity risk (World Health Organization, 2010) and adverse health conditions later in life (Krebs & Jacobson, 2003). Relatively few studies have explored factors that influence adolescent mothers' infant feeding practices or useful learning modalities. The aim of the exploratory study reported here was to add to the current body of knowledge in the identification of: (1) factors affecting low-income adolescent mothers' infant feeding practice and (2) useful learning strategies. Extension professionals are well positioned to provide nutrition education to adolescent mothers.
Literature Review
The theory of planned behavior served as the framework for the study. According to this theory, attitudes, subjective norms, and perceived behavior control influence behavioral intentions and ultimately predict behavior (Ajzen, 1985). This framework allowed us to examine multiple factors that may influence infant feeding practices in low-income adolescent mothers.
Attitudes
Behavioral beliefs and evaluations of behavioral outcomes influence attitudes toward a specific behavior. Adolescent mothers are often unprepared for the tasks of parenting. These mothers struggle with negotiating both the developmental tasks of adolescence as well as being a parent (Brosh, Weigel, & Evans, 2009; Hess, Papas, & Black, 2002). Compared to adult mothers, adolescent mothers are less knowledgeable, less responsive, more controlling, and less skilled in infant feeding (Garcia Coll, Vohr, Hoffman, & Oh, 1986), which interferes with infants' self-regulation, natural weight trajectory, and healthy growth during the first year of life (Taveras et al., 2004). Factors such as an infant's temperament, size, and appetite can influence adolescent mothers' attitudes toward infant feeding, which can result in unhealthy feeding practices (Contreras & Horodynski, 2010; Heinig et al., 2006; Horodynski et al., 2007; Worobey, Lopez, & Hoffman, 2009).
Subjective Normative Beliefs
Normative beliefs and the motivation to comply contribute to the development of subjective norms. Adolescent mothers are in need of and actively seek guidance from others (Letourneau, Stewart, & Barnfather, 2004). Adolescent mothers' subjective norms surrounding infant feeding may be influenced by cultural beliefs/practices and advice from family members, friends, or health care/Extension professionals. Bentley, Gavin, Black, and Teti (1999) reported that infants' maternal grandmothers are often the primary decision-makers for low-income African American adolescents regarding infant feeding. DeVito (2007) also found that adolescent mothers identified their own mothers as their primary support person.
Perceived Behavior Control
Perceived behavior control comprises control beliefs and perceived power. Adolescent mothers often struggle as they try to navigate staying in school, working, and caring for their infant (Letourneau et al., 2004). There are a variety of services and resources available to assist and support adolescent mothers through the government, community/Extension programs, and nonprofit agencies (Kulkarni, Kennedy, & Lewis, 2010); however, barriers exist for adolescent mothers in accessing these resources. Family, partners, and friends were reported to be the most relied-upon sources of support for this population (Letourneau et al., 2004). Reliance on others to provide financial support and/or infant care may limit the adolescent mother's perceived control over infant feeding decisions.
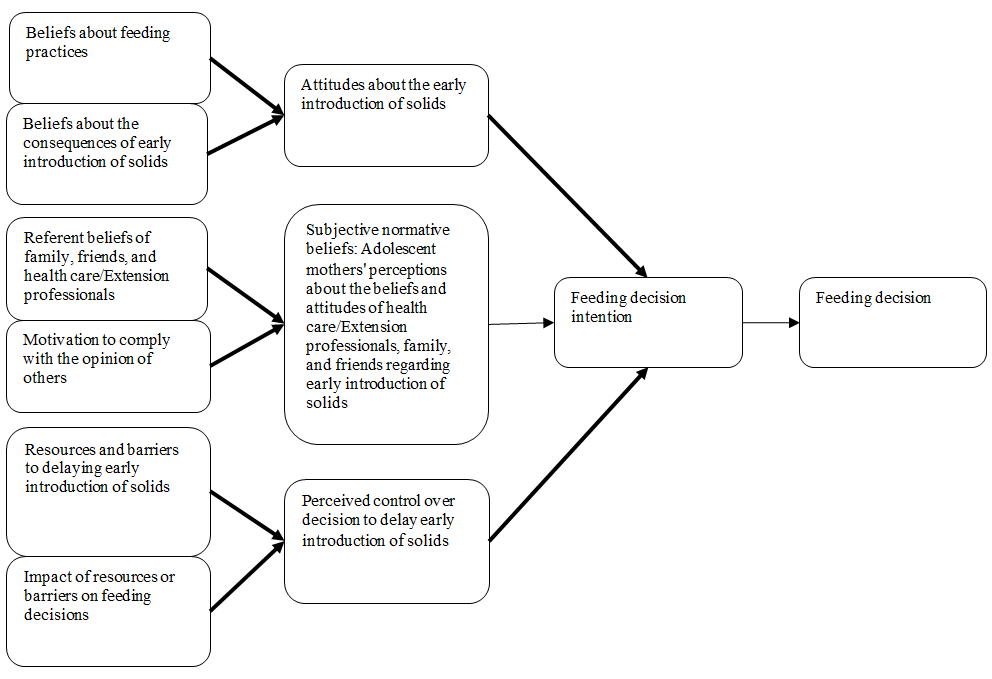
Conceptual Model
Our conceptual model was an adaptation of Brophy-Herb, Silk, Horodynski, Mercer, and Olson's (2009) infant feeding decisions framework (Figure 1).
Figure 1.
Conceptual Model for Infant Feeding Practices
Methodology
Two focus groups were conducted in 2011 in two Michigan communities with low-income adolescent mothers of infants (n = 9 at site one [n = 8 African American (AA), n = 1 non-Hispanic white (NHW)]; n = 7 at site two [n = 6 NHW, n = 1 AA]).
Recruitment
Participants were recruited through a community teen program for adolescent mothers in one community and through an Extension nutrition program in another community. The research team obtained written parental consent for both the adolescent to be contacted and to participate in the study, as well as adolescent assent for voluntary participation in the study. Adolescent mothers received a $50 honorarium for their participation in the focus group. The study was approved by the Michigan State University Committee on Research Involving Human Subjects.
Inclusion criteria for the two focus groups were: (a) low-income adolescent first-time mothers aged 15 to 19 years who were at or below the 185% U.S. federal poverty index level; (b) English speaking; (c) a primary caregiver for infant feeding; (d) self-identified as AA or NHW; (e) singleton birth; and (f) infant between the ages of 0 to 12 months. The researchers acknowledge the broad age span for the infants; the selection was based on the accessibility of recruitment within this population and the intent to include mothers of infants who had already introduced solid foods.
Focus Group Procedure
Focus groups were held at community sites where adolescent mothers attended Extension/teen programs. Following a semi-structured guide designed to elicit adolescent mothers' perceptions and practices regarding infant feeding, sources of information/advice about infant feeding, and useful learning strategies, one trained moderator facilitated the 90-minute audio-recorded focus groups, and one project manager took supplemental notes. Questions with prompts were developed and reviewed for clarity by the research team (Table 1) and for cultural appropriateness by two women under the age of 21, one AA and one NHW.
| Questions |
|
Analytic Approach
Audiotapes were transcribed verbatim by a professional, and content analysis was conducted as an iterative process. The principal investigator and a graduate research assistant evaluated the responses from the focus groups and identified major content areas independently. The reviewers met to discuss general impressions, refine the text into specific coding categories, and formulate themes. NVivo, a qualitative software program that facilitates coding, searching, and retrieving of data, was used.
Results
Participant Characteristics
Of the 16 participants, none were married, the majority reported being in a relationship (n = 14, 88%), with three living with a partner; 44% (n = 7) had completed high school; and the majority were not working (n = 13, 81%). More than four-fifths of the infants (n = 14, 88%) were currently receiving formula. Half (n = 8, 50%) reported never initiating breastfeeding, with 31% (n = 5) switching to formula when the baby was less than 1 week old; 56% ( n = 9) breastfed for less than 1 month; and 19% ( n = 3) breastfed for 1 to 2 months. The mean age of infants was 7 months, with an average birth weight of 6 pounds, 7 ounces.
Focus Group Findings
Three themes emerged from content analysis of the data which add to the current body of knowledge on adolescent mothers' infant feeding practices: (1) feeding decisions related to introduction of solid foods; (2) feeding information/advice provided by others; and (3) useful learning strategies (Table 2).
Theme one was conceptualized as adolescent mothers' infant feeding behaviors and decisions regarding introducing solid foods. A major reason adolescent mothers gave for beginning early introduction of solid foods, that is, before the American Academy of Pediatrics (AAP) recommendation of introducing solid foods at age 4-6 months [2012]), was based on their perception that formula alone was not sufficient to fill their babies up. Similarly, adolescent mothers lacked knowledge of how much formula or breast milk their babies needed.
Theme two was conceptualized as the type, source, and relative importance of feeding advice given to the teen moms. Adolescent mothers received advice from a variety of sources, and advice from the teen's mother meant the most, particularly for AA teens. Adolescent mothers claimed that advice from health care/Extension professionals was helpful, but when asked how often they followed this advice, responses ranged from not following most of it to following as much as they could. Mothers sometimes stated that advice from their health care/Extension professionals differed from the advice of their family members. Another variable was other persons who fed the infant (e.g., family members or friends). Oftentimes, others fed the infant inappropriate foods or liquids before the baby was 4 months old. The mothers were not concerned about infant obesity or the later health risks associated with obesity.
Theme three was conceptualized as the learning strategies adolescent mothers identified as helpful and useful in learning about infant feeding. Teens gave a variety of ways in which they would like to receive information on infant feeding, such as text messaging, Facebook, emailed newsletters, and home visits. Useful information on infant feeding included: (a) when to start feeding solids, (b) what types of solids to start with, (c) frequency of feeding, (d) how to identify satiety cues, and (e) when to discontinue formula and start on whole milk. Participants indicated information should be given in short lessons with key points to maintain attention.
| Theme | Sub-Theme | Supporting Data |
| Feeding decisions related to introduction of solid foods | Formula or breast milk as insufficient | "…some babies do not get full off what they eat, and they have to start solid foods even if they are not old enough…" "…My baby is 3 months and I did give him way too much (formula) one time. So…I decided to drop the formula 'cause he was doing 7 ounces, so I dropped his formula and started feeding him baby food. And that was so I didn't have to give him so much formula every time." |
| Feeding information/advice provided by others | Valuing mother's advice | "…I think I'd go with what my mom says. And if I feel iffy about it, maybe I'd look it up. But I usually go with what my mom says, and then the doctor. But then if I still feel it's not right, I'll go with my own instinct." "I make decisions about what my baby eats or drinks but I like to go to my mom first, and ask her…" |
| Advice of health care/Extension professionals | "…I don't feel like the stuff the health professionals tell me is right." "…Yes, I trust some of the information from the health professionals, like when they say not to give your baby hot dogs; but when they say things about not drinking juice, I don't think that is right…" "…The only thing I haven't followed was waiting to start my baby on solid foods. My doctor told me to wait, but she is almost 4 months and bottles did not seem to fill her up enough so I give her jar food." | |
| Other influences | "…My parents decided it would be cool to give my 4 month old daughter ice cream and then she got sick and I had to deal with that, and I was mad" "…My aunt…not gonna put her down like this, but, she's bad. She gave jar foods and stuff… and my baby is only 2 months old" | |
| Concerns about obesity | "No, I think she will grow out of her chubbiness when she gets older…" "…I don't believe in babies being too fat…but I can see if he was a 3-year-old…" "I'm not concerned at all, 'cause my baby was big when he was born, so I'm not worried…" | |
| Useful learning strategies | Information to receive | "…knowing how much formula to give them and how often…" "…how do you do formula with solid food…" |
| Strategies to use | "Internet"; "…text messages and apps…" "Lessons should only last about 30 minutes or less because if it goes on for like an hour I won't pay attention 'cause I'll get too bored" |
Conclusion
Limited research exists that examines factors affecting low-income adolescent mothers' infant feeding practices and useful learning modalities. The exploratory study reported here identified themes that can be used by Extension professionals in designing nutrition education interventions for this population. The study results are consistent with the theory of planned behavior in which attitudes, subjective normative beliefs, and perceived control appear to influence adolescent mothers' feeding intentions and ultimately their feeding decisions (Figure 2).
Understanding adolescent mothers' attitudes, subjective normative beliefs, and perceived control with regard to infant feeding decisions provides insight into promoting adherence to the AAP recommendation to introduce solid food no earlier than 4 to 6 months of age. Data revealed that some adolescent mothers do not participate in the healthiest infant feeding practices because of inaccurate or inadequate advice or lack of knowledge. The study's findings add to the current body of knowledge and provide additional insight and understanding into adolescent mothers' infant feeding practices that are evidenced-based versus common sense assumptions and thus provide insight critical in developing programs to improve infant health in support of Healthy People 2020 (USDHHS) recommendations. Healthy People 2020 promotes implementing multidisciplinary public health interventions that address fostering healthy eating habits as early childhood sets the stage for later eating habits. Our findings provide guidance for Extension professionals in the development of targeted interventions with adolescent mothers using proposed learning strategies based on this recommendation.
Figure 2.
Conceptual Model for Infant Feeding Practices for Low-Income Adolescent Mothers
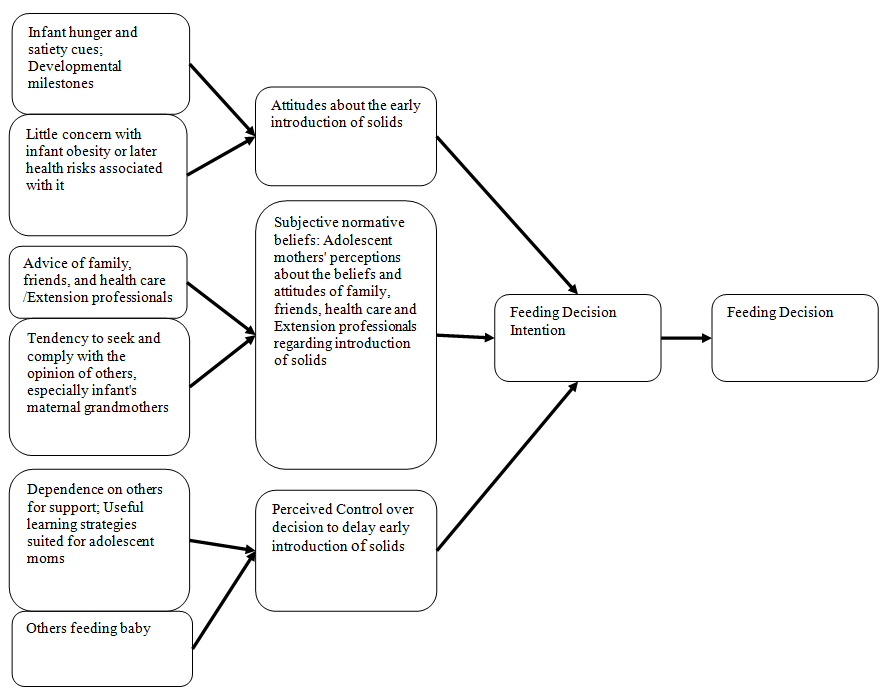
Beliefs about feeding practices appeared to influence attitudes regarding early introduction to solid foods. Many adolescent mothers thought that their babies were not getting enough to eat and began introducing solid foods prior to AAP recommendations. Adolescent mothers want their babies to be "full" and "not hungry" and thus may misread the baby's cues, resulting in premature introduction of solid foods or overfeeding. Adolescent mothers who are unaware of appropriate infant developmental milestones often believe that their infant is more developmentally mature than what is generally considered age-acceptable (e.g., able to hold a cup or spoon, sitting up) (Carruth, Nevling, & Skinner, 1997; Karp & Lutenbacher, 2011). Attitudes also appeared to be influenced by beliefs about the lack of consequences of early introduction of solid foods. Adolescent mothers did not seem to be concerned about obesity during infancy or the later health risks associated with childhood obesity.
Subjective normative beliefs were shaped by referent beliefs of others. While some mothers followed the advice of health care/Extension professionals, adolescent mothers frequently determined when to start solid foods, the amount and type of solid foods, and the amount and type of liquids based upon the advice of non-professionals. This may be indicative of adolescent mothers' motivation to comply with the opinions of others.
Perceived control in delaying the early introduction of solid foods may also be influenced by the presence or absence of resources and/or barriers. These mothers had some access to resources as they were recruited from community/Extension programs. Useful learning strategies for learning about infant feeding should be adapted to suit the lives of adolescent mothers. To reduce the risk of childhood obesity, new methods must be adapted to the learning and information-seeking styles preferred by frequent technology users (Ahern, Phalen, Le, & Goldman, 2007). Perceived control may also be influenced by adolescent mothers' dependence on others for support and feeding the baby. Adolescent mothers are especially at risk due to limited experience with infant feeding and often are dependent on their mother or other close family members for guidance (Black, Siegel, Abel, & Bentley, 2001).
While such findings shed additional knowledge on adolescent mothers' infant feeding practices, the research is limited by the small sample size and single case studied. Continued investigations into interventions needed to help adolescent mothers learn and adopt new knowledge, attitudes, and skills regarding infant feeding should be conducted. Cultural beliefs and messages should be considered as these may increase the amount of conflicting information received from professionals versus lay persons (Ontai, & Mastergeorge, 2006; Ontai, Williams, Lamp, & Smith, 2007). Related research should include use of social media as a strategy to inform and/or assist adolescent mothers with healthy infant feeding practices.
Acknowledgements
Funding for the research reported here was provided by the Alpha Psi Chapter of Sigma Theta Tau International Honor Society of Nursing, Inc. The Principal Investigator would like to express gratitude to: the adolescent mother focus group participants; Ms. Lindsay Neuberger for her help with the focus groups; and Ms. Amanda Diemert for her assistance with data analysis. The authors also acknowledge their research team, Drs. Kami Silk and Holly Brophy-Herb, for their contribution to the research project.
References
Ahern, D. K., Phalen, J. M., Le, L. X., & Goldman, R. E. (2007). Childhood obesity prevention and reduction: Role of eHealth. Boston, MA: Health e-Technologies Initiative. Retrieved from: http://www.hetinitiative.org/Childhood%20Obesity%20Prevention%20and%20Reduction%20-%20Role%20of%20eHealth.pdf
Ajzen, I. (1985). From intentions to actions: A theory of planned behavior. In J. Kuhl & J Beckmann (Eds.), Action Ccontrol: From cognition to Bbehavior (pp. 11–39). Heidelberg, Germany: Springer Berlin Heidelberg.
American Academy of Pediatrics. (2012). Switching to solid foods. Retrieved from: http://www.healthychildren.org/English/ages-stages/baby/feeding-nutrition/pages/Switching-To-Solid-Foods.aspx
Bentley, M., Gavin, L., Black, M. M., & Teti, L. (1999). Infant feeding practices of low-income, African-American, adolescent mothers: An ecological, multigenerational perspective. Social Science & Medicine, 49(8), 1085–1100. doi: 10.1016/S0277-9536(99)00198-7
Black, M. M., Siegel, E. H., Abel, Y., & Bentley, M. E. (2001). Home and videotape intervention delays early complementary feeding among adolescent mothers. Pediatrics, 107(5), 67–174. doi: 10.1016/S0277-9536(99)00198-7
Brophy-Herb, H. E., Silk, K., Horodynski, M. A., Mercer, L., & Olson, B. (2009). Key theoretical frameworks for intervention: understanding and promoting behavior change in parent–infant feeding choices in a low-income population. Journal of Primary Prevention, 30(2), 191–208. doi: 10.1007/s10935-009-0169-9
Brosh, J., Weigel, D., & Evans, W. (2009). Assessing the supports needed to help pregnant and parenting teens reach their educational and career goals. Journal of Extension [On-line], 47(1), Article 1RIB8. Available at: http://www.joe.org/joe/2009february/rb8.php
Carruth, B. R., Nevling, W., & Skinner, J. D. (1997). Developmental and food profiles of infants born to adolescent and adult mothers. Journal of Adolescent Health, 20(6), 434–441. doi: 10.1016/S1054-139X(97)00034-7
Contreras, D. A., & Horodynski, M. A. (2010). The influence of parenting stress on mealtime behaviors of low-income African-American mothers of toddlers. Journal of Extension [On-line], 48(5), Article 5RIB3. Available at: http://www.joe.org/joe/2010october/rb3.php
DeVito, J. (2007). Self-perceptions of parenting among adolescent mothers. The Journal of Perinatal Education, 16(1), 16–23. doi: 10.1624/105812407X170680
Garcia Coll, C., Vohr, B. R., Hoffman, J., & Oh, W. (1986). Maternal and environmental factors affecting developmental outcome of infants of adolescent mothers. Journal of Developmental and Behavioral Pediatrics, 7(4), 230–236.
Heinig, M. J., Follett, J. R., Ishii, K. D., Kavanagh-Prochaska, K., Cohen, R., & Panchula, J. (2006). Barriers to compliance with infant-feeding recommendations among low-income women. Journal of Human Lactation, 22(1), 27-38. doi: 10.1177/0890334405284333
Hess, C. R., Papas, M. A., & Black, M. M. (2002). Resilience among African American adolescent mothers: Predictors of positive parenting in early infancy. Journal of Pediatric Psychology, 27(7), 619–629. doi: 10.1093/jpepsy/27.7.619
Horodynski, M., Olson, B., Arndt, M.J., Brophy-Herb, H., Shirer, K., & Shemanski, R. (2007). Low-income mothers' decisions regarding when and why to introduce solid foods to their infants: Influencing factors. Journal of Community Health Nursing, 24(2), 101–118. doi: 10.1080/07370010701316247
Karp, S. M., & Lutenbacher, M. (2011). Infant feeding practices of young mothers. MCN: The American Journal of Maternal/Child Nursing, 36(2), 98–103. doi: 10.1097/NMC.0b013e31820558bf
Krebs, N. F., & Jacobson, M. S. (2003). Prevention of pediatric overweight and obesity. Pediatrics, 112(2), 424–430.
Kulkarni, S. J., Kennedy, A. C., & Lewis, C. M. (2010). Using a risk and resilience framework and feminist theory to guide social work interventions with adolescent mothers. Families in Society, 91(3). 217–224. doi: 10.1606/1044-3894.3998
Letourneau, N. L., Stewart, M. J., & Barnfather, A. K. (2004). Adolescent mothers: Support needs, resources, and support-education interventions. Journal of Adolescent Health, 35(6), 509–525. doi:10.1016/S1054-139X(04)00069-2
Mihrshahi, S., Battistutta, D., Magarey, A., & Daniels, L. A. (2011). Determinants of rapid weight gain during infancy: Baseline results from the NOURISH randomised controlled trial. BMC Pediatrics, 11, 99. doi: 10.1186/1471-2431-11-99
Ontai, L. L., & Mastergeorge, A. M. (2006). Culture and parenting: A guide for delivering parenting curriculums to diverse families. Journal of Extension [On-line], 44(4), Article 4TOT5, Available at: http://www.joe.org/joe/2006august/tt5.php
Ontai. L. L., Tierney Williams, S., Lamp, C., & Smith, D. (2007). An integrative approach to addressing childhood overweight: Inclusion of parenting information in nutrition education programs. Journal of Extension [On-line], 45(3), Article 3FEA2. Available at: http://www.joe.org/joe/2007june/a2.php
Taveras, E. M., Scanlon, K. S., Birch, L., Rifas-Shiman, S. L., Rich-Edwards, J. W., & Gillman, M. W. (2004). Association of breastfeeding with maternal control of infant feeding at age 1 year. Pediatrics, 114(5), e577–e583. doi: 10.1542/peds.2004-0801
U.S. Department of Health and Human Services. Office of Disease Prevention and Health Promotion. Healthy People 2020. Washington, DC. Retrieved from: http://www.healthypeople.gov/2020/topicsobjectives2020/. Accessed 6/4/14.
World Health Organization. (2010). Population-based prevention strategies for childhood obesity: Report of the WHO forum and technical meeting. Geneva, Switzerland: World Health Organization.
Worobey, J., Lopez, M. I., & Hoffman, D. J. (2009). Maternal behavior and infant weight gain in the first year. Journal of Nutrition Education and Behavior, 41(3), 169–175. doi: 10.1016/j.jneb.2008.06.005