August 2013
|
August 2013 // Volume 51 // Number 4 // Feature // v51-4a2



Strength Training Improves Body Image and Physical Activity Behaviors Among Midlife and Older Rural Women
Abstract
The effect of strength training on body image is understudied. The Strong Women Program, a 10-week, twice weekly strength-training program, was provided by Extension agents to 341 older rural women (62±12 years); changes in body image and other psychosocial variables were evaluated. Paired-sample t-test analyses were conducted to assess mean differences pre- to post-program. Strength training was associated with significant improvements in several dimensions of body image, health-related quality of life, and physical activity behaviors, satisfaction, and comfort among rural aging women—an often underserved population that stands to benefit considerably from similar programs.
Purpose
Physical activity is essential to maintaining health, wellness, and physical function, particularly as people age, yet individuals over the age of 50 are more sedentary than any other segment of the adult population (Haskell et al., 2007; He & Baker, 2004; Nelson et al., 2007; von Bonsdorff & Rantanen, 2011). Strength training participation, in particular, is an important element of physical activity for midlife and older women because it helps women maintain muscle and bone mass and reduces risk for numerous chronic diseases.
Research indicates that exercise confers benefits to many dimensions of health, including physical, emotional, intellectual, and social wellness, such as improved sleep, quality of life, and mental health (Penedo & Dahn, 2005; Singh, Clements, & Fiatarone, 1997a, 1997b; Stephenson, 2012). However, much of the exercise research has focused on aerobic activity rather than strength training, and few studies have specifically focused on body image among aging women.
Poor body image is commonly reported among younger women, but research suggests that body image perceptions may also be low in older women (Peat, Peyerl, & Muehlenkamp, 2008). Poor body image and body dissatisfaction are of concern in older women as evidenced by their association with disordered eating, dieting, smoking, and cosmetic surgery (Grogan, Fry, Gough, & Conner, 2009; Haas, Champion, & Secor, 2008; Peat et al., 2008). Dieting and restrained eating may also lead to slower cognitive performance, which is of particular concern in older populations (Green & Rogers, 1995). A more positive body image is associated with better self-esteem, quality of life, physical and emotional well-being, social competence, and self-care and with decreased rates of depression and anxiety (McLean, Paxton, & Wertheim, 2010; Slevec & Tiggemann, 2011). In addition, negative body image can be a barrier to participation in physically active leisure activities (Allender, Cowburn, & Foster, 2006).
Research also shows that social support and access to locations and opportunities, as well as many other factors, are important in engaging rural older adults in physical activity (Kruger, Murray, & Zanjani, 2011; Fitzgerald & Spaccarotella, 2009; Wilcox, Castro, King, Housemann, & Brownson, 2000). Thus, increasing opportunities for rural aging women to participate in supportive, community-based exercise programs hold substantial potential to affect positive changes in many dimensions of health (physical, mental, and emotional) among this population (Pratt & Bowman, 2008; Kang & Russ, 2009).
The Strong Women Program (SWP) is an evidence-based, community strength training program specifically targeted to women aged 40 and older, with the goals of helping them maintain their strength, function, and independence (Seguin et al., 2008). The SWP focuses on increasing women's access to regular strength training opportunities and increasing their knowledge about the importance of regular strength training (Seguin et al., 2008). SWP has been successfully implemented by local Extension Family and Consumer Sciences agents whose expertise is providing research-based, community wellness programs (Pratt & Bowman, 2008; Young, Weinert, & Spring, 2012).
Prior research with SWP participants has demonstrated significant pre-post changes across several parameters of physical fitness, including strength, agility, aerobic fitness, and flexibility (Seguin, Heidkamp-Young, Kuder, & Nelson, 2012). The present research aimed to evaluate pre-post changes in body image, other psychosocial variables, and physical activity behavior to further understand the range of potential benefits among rural aging women.
Methods
Participants
Participants were 341 female residents (94% Caucasian) from nine Montana counties. Their age range was 23-87 years (mean±SD = 62±12). Four percent of the women were under the age of 40, 37% were 40-59, and 59% were 60 years old or older. Average population density of the nine counties is approximately 13 people per square mile, compared to an average national county density of 86 people per square mile (USDA Economic Research Service, 2009).
The Program
The SWP classes last approximately 1 hour and consist of 5 minutes of warm up (e.g., walking, marching in place), 40 minutes of strength training, 5 minutes of balance training, and 5 minutes of cool down (i.e., stretching and flexibility exercises). It is recommended that SWP sessions ideally last 8 to 12 weeks, with two 60-minute classes per week on nonconsecutive days with encouragement for participants to engage in the activities at home once weekly (Seguin et al., 2008; Seguin et al., 2012). For the study reported here, the SWP was taught by Montana State University Extension Family and Consumer Sciences agents at 14 sites across the nine counties. The length of sessions varied from 4 to 12 weeks, with the majority running 10 weeks. The number of participants per county also varied; some counties offered one session, while others offered multiple sessions. Participants per country ranged from seven (one site, one session) to 94 (several sites, multiple sessions), with an average of 32 participants per country.
Measures
At pre- and post-session individual appointments, participants completed questionnaires designed to collect information on several outcomes of interest: psychosocial factors, including body image, and physical activity behavior. Tufts University, in close collaboration with partnering institutions across the U.S. (in the case of the study reported here, Montana State University), conducts ongoing research related to the StrongWomen Program. All materials and procedures for the research were approved by the Tufts University Human Investigation Review Board (#7049).
The Multidimensional Body-Self Relations Questionnaire (MBSRQ) assesses multiple attitudinal aspects of body image (Andresen, Fouts, Romeis, & Brownson, 1999; Brown, Cash, & Mikulka, 1990). This validated self-evaluation measure was designed to assess cognitive, behavioral, perceptual, affective, and subjective views about one's body (Thompson, Heinberg, Altabe, & Tantleff-Dunn, 1999). The six subscales (36 total items) used included the following:
- Fitness Evaluation (3 items)
- Fitness Orientation (13 items)
- Health/Illness Evaluation (6 items)
- Health/Illness Orientation (8 items)
- Weight Preoccupation (4 items)
- Self-Classified Weight (2 items)
For Fitness and Health/Illness statements, participants respond using a 5-point scale ranging from 1 (definitely disagree) to 5 (definitely agree). For Self-Classified Weight statements, respondents choose from 1=very underweight, 2=somewhat underweight, 3=normal weight, 4=somewhat overweight, 5=very overweight. The Weight Preoccupation question asks about frequency of crash diets, with the following answer options 1=never, 2=rarely, 3=sometimes, 4=often, 5=very often.
Health-related quality of life was measured using the Centers for Disease Control and Prevention (CDC)'s four-item set of HRQOL questions (Centers for Disease Control and Prevention, 2000). The four HRQOL questions are: (1) "Would you say that in general your health is excellent, very good, good, fair, or poor?"; (2) "Now thinking about your physical health, which includes physical illness and injury, for how many days during the past 30 days was your physical health not good?" (physically unhealthy days); (3) "Now thinking about your mental health, which includes stress, depression, and problems with emotions, for how many days during the past 30 days was your mental health not good?"(mentally unhealthy days); and (4) "During the past 30 days, for about how many days did poor physical or mental health keep you from doing your usual activities, such as self-care, work, or recreation?" (activity-limiting days). The "unhealthy days" measures have been validated in several population studies (Andresen et al., 1999; Moriarty, Zack, & Kobau, 2003; Ounpuu, Krueger, Vermeulen, & Chambers, 2000). They have also been used by the CDC in the Behavioral Risk Factor Surveillance System (BRFSS) surveys since 1993 and in the National Health and Nutrition Examination Survey since 2000 (Moriarty et al., 2003).
Additionally, participants answered questions about comfort level with exercise (2 items). Specifically, they are asked (1) if they are comfortable with their current level of physical activity and (2) if they are comfortable increasing their level of physical activity. The comfort scale, developed by Cardello and colleagues, ranges from -100 (greatest imaginable discomfort) to +100 (greatest imaginable comfort) (Cardello, Winterhalter, & Schutz, 2003).
The Physical Activity Questionnaire, previously used in the Steps to a New You program was used to assess physical activity behavior and satisfaction (Pelican, Paul, Raidl, Gossett, & Lanting, 2006). The first three questions ask about times per week participants engaged in moderate physical activity, stretching, and strength-training, with seven possible answers ranging from 0 to 7 times per week. The two statements "I enjoy being physically active" and "I get as much physical activity as I need" are scored on a five-point scale ranging from 1 (strongly disagree) to 5 (strongly agree). Additionally, there are two questions related to sedentary behavior; these ask about the number of hours per weekend day and per weekday of television viewing. The 5-point scale for these questions ranged from 1 (8 hours or more) to 5 (1 hour or less).
Exercise logs were used by women during each session to keep track of the amount lifted for the six exercises for which hand weights (dumbbells) or adjustable ankle weights were used. Progression is an important component of a strength training program. Participants in the SWP are encouraged to slowly and safely increase the intensity of the exercises (or the amount of weight they are lifting) to help them continue to improve strength and related benefits.
Analysis
Individual pre- and post-program evaluation scores were used to calculate pairwise t-tests for each dependent variable (DV). The pre- and post-program group means, mean change, 95% confidence interval and p-value associated with each DV are shown in Tables 1-3, where p-values < 0.05 are considered significant.
Results
Average percent attendance of the classes was 74±19. Although 341 women participated, not every participant completed pre- and post-program questionnaires and/or exercise logs. Overall, the women progressed in terms of intensity in the exercise program, and they improved across several behavioral and psychosocial outcomes following participation in the 10-week community-based exercise program.
Participants significantly increased the weight lifted for all exercises in which hand weights or adjustable ankle weights are used. The complete list of exercises, the order in which they were completed, and the participants' pre-post weights lifted are shown in Table 1.
| Strength Training Exercise | Pre-Test (lbs) (Mean) | Post-Test (lbs) (Mean) | Change (lbs) (±SD) | N | 95% CI | p-value |
| Wide leg squat* | - | - | - | - | - | - |
| Standing leg curl | 2.1 | 4.7 | 2.6 (± 2.4) | 218 | 2.3, 3.0 | <0.001 |
| Knee extension | 2.1 | 4.8 | 2.7 (± 2.5) | 209 | 2.4, 3.1 | <0.001 |
| Standing side hip/leg raise | 2.1 | 4.6 | 2.4 (±2.5) | 228 | 2.1, 2.7 | <0.001 |
| Biceps curl | 2.6 | 5.4 | 2.8 (± 2.1) | 261 | 2.5, 3.0 | <0.001 |
| Overhead press | 2.6 | 4.9 | 2.3 (± 2.0) | 252 | 2.0, 2.5 | <0.001 |
| Bent forward fly | 2.3 | 3.9 | 1.6 (± 1.6) | 225 | 1.5, 1.9 | <0.001 |
| Toe stand* | - | - | - | - | - | - |
|
* These two exercises use body weight instead of dumbbells or adjustable ankle weights; they are shown here to be inclusive of all exercises that are completed. All exercises in the program are shown above in the order in which they are completed in the program. |
||||||
Six categories from the MBSRQ were assessed in the study, as shown in Table 2. At the conclusion of the program, the women had significantly improved on body image scores for Health Orientation, Subjective Weight, Fitness Orientation, Fitness Evaluation, and Health Evaluation. There was no change in Weight Preoccupation. Participants also reported a small but significant improvement in the General Health measure within the HRQOL (pre-test score=3.45; post-test score=3.55; p=0.02); there were no changes in the other measures of the HRQOL (data not shown).
| Body Image Dimension | Pre-Test (Mean) | Post-Test (Mean) | Change (± SD) | N | 95% CI | p-value |
| Health Orientation* | 3.69 | 3.74 | 0.06 (± 0.45) | 254 | 0.00, 0.11 | 0.048 |
| Subjective Weight† | 3.76 | 3.64 | 0.12 (± 0.54) | 224 | 0.05, 0.19 | 0.001 |
| Fitness Orientation* | 3.20 | 3.44 | 0.24 (± 0.44) | 223 | 0.19, 0.30 | <0.001 |
| Fitness Evaluation* | 3.18 | 3.28 | 0.10 (± 0.61) | 227 | 0.02, 0.18 | 0.017 |
| Health Evaluation* | 3.65 | 3.73 | 0.07 (± 0.43) | 226 | 0.02, 0.13 | 0.009 |
| Weight Preoccupation‡ | 2.75 | 2.74 | 0.01 (± 0.55) | 225 | -0.06, 0.08 | 0.811 |
|
* Higher or increasing score is better for this scale. †A score of 3 is "normal"; thus, change in the direction of a score of 3 is a positive change. ‡ Lower or decreasing score is better for this scale. |
||||||
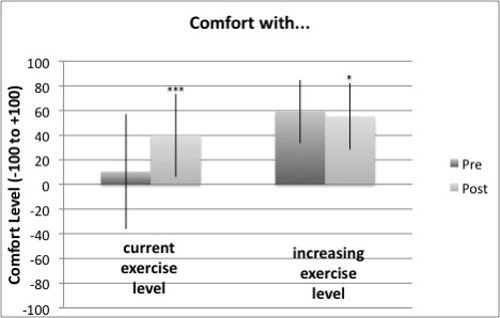
Participants also reported engaging in significantly more frequent moderate physical activity, stretching, and strength training compared to when they started the program. They reported significantly higher levels of physical activity satisfaction—feeling increased levels of enjoyment for physical activity and feeling that they are getting enough physical activity (Table 3). Shown in Figure 1, there was a statistically significant positive increase in comfort with current level of exercise pre- to post-test (item 1). The magnitude of the change was about 30 scale points. In the case of comfort with increasing exercise level (item 2), on the other hand, there was a small but statistically significant decrease in comfort from pre- to post-test. In this case, the decrease was from a relatively high level of positive comfort (59.37) to a slightly lower, but still positive, level (55.01). Despite the fact that on average item 1 tended to increase while item 2 tended to decrease (from pre- to post-test), these scores were strongly positively correlated (r=0.284, p<.001).
| Characteristic | Pre- Test (Mean) | Post- Test (Mean) | Change (± SD) | N | 95% CI | p-value |
| Physical Activity Category (times/week) | ||||||
| Moderate Physical Activity | 3.53 | 4.26 | 0.72 (± 1.52) | 235 | 0.53, 0.92 | <0.001 |
| Stretching | 1.79 1.08 | 2.93 2.47 | 1.14 (± 1.73) | 235 | 0.092, 1.36 | <0.001 |
| Strength Training | 1.08 | 2.47 | 1.39 (± 1.57) | 235 | 1.19, 1.60 | <0.001 |
| Physical Activity Satisfaction (1=strongly disagree, 5=strongly agree) | I enjoy being physically active | 4.30 | 4.42 | 0.113 (± 0.68) | 234 | 0.03, 0.20 | .012 | I get as much physical activity as needed | 2.36 | 2.85 | 0.485 (± 0.83) | 234 | 0.38, 0.59 | <0.001 |
Figure 1.
Change in Participants' Comfort with Exercise Level
Discussion
Prior research has demonstrated fitness benefits of this community-based strength training program targeted to midlife and older women (Seguin et al., 2012). The present study is the first to demonstrate improvements in body image, health-related quality of life, personal satisfaction, and comfort about physical activity levels as well as physical activity behaviors.
Both experimental and observational studies indicate that exercise has a positive impact on dimensions of body image, including perceived physical appearance, body self-concept, and social physique anxiety (Campbell & Hausenblas, 2009; Hausenblas, Janelle, Gardner, & Hagan, 2003; Tiggemann, 2004). A 2007 meta-analysis by Reel and colleagues also found that weight training more positively affected body concerns than aerobic-type exercises (Reel et al., 2007). Although prior studies examining the effects of strength training on body image have demonstrated improvements, the majority of these studies have been conducted with pre-adolescents, adolescents, or young adults (Ahmed, Hilton, & Pituch, 2002; Caruso & Gill, 1992; Duncan, Al-Nakeeb, & Nevill, 2009; Lubans & Cliff, 2011; Lubans, Sheaman, & Callister, 2010; Martin Ginis, Eng, Arbour, Hartman, & Phillips, 2005).
Only three studies were identified that have examined the effects of strength training programs on body image in middle aged and older adults, with mixed results. Tucker and colleagues found that middle-aged women who participated in a resistance training program improved their body image perceptions significantly more than those in a walking program (Tucker & Mortell, 1993), and more recently, a study by Speck and colleagues reported that twice-weekly strength training for 1 year resulted in significantly greater improvement in body image in a strength-training versus control group among female breast cancer survivors (Speck et al., 2010). However, Shaw and colleagues found no differences in perception of physical appearance between the exercise and control group participants following nine months of strength training (Shaw, Ebbeck, & Snow, 2000). Collectively, these studies indicate that strength training may improve body image among aging women, but the data are not conclusive, and the number of studies is quite limited. Thus, data from the present study add to this literature, demonstrating that several dimensions of body image are sensitive to change among older rural women, including positive shifts in attitudes and beliefs about their weight, fitness, and health.
We know that small increases in time spent being active cumulatively add up to important health benefits (Haskell et al., 2007). Analysis of data from the 2001 BRFSS survey found that adults who engaged in recommended levels of physical activity were significantly less likely to report 14 or more unhealthy days for each of the unhealthy day measures compared to physically inactive adults. These associations were observed across all age groups, although the associations tended to be stronger in adults aged 45 years or older (Brown et al., 2003; Brown et al., 2004). In the present study, data from three physical activity behaviors—general physical activity, stretching, and strength training—all improved, which is a positive indication of healthy lifestyle progress in this population. Future research may benefit from using objective pre-post measures (e.g., accelerometers) of physical activity behavior change during and following strength training program participation in similar populations.
Another important element of change in the present study is the positive shift towards enjoying exercise more. The women still report only moderate success (post-test: 2.85 out of 5) in terms of getting enough exercise, but it is an improvement in the right direction. This finding is reinforced by participants' reported feelings of comfort about their current physical activity level pre and post program, which increased 30 points (out of 200). Mentally, they are feeling more positive about exercise and more positive about themselves in terms of how much exercise they are participating in. We also know that it can be difficult for people to initiate change and maintain it (Seguin et al., 2008). The retention rate was nearly 80%, and the program clearly provided important knowledge and tools to help the women move towards being more active in general, enjoying exercise more, and feeling more comfortable with physical activity. The high retention rate also lends support to the benefits of social settings, including exercising with others and a positive learning environment created by the program facilitators.
Quality of life during the later years has also been found to be as important as duration of life for many older individuals (Branch, 1985). In the study reported here, women improved significantly only on the "General Health" category of the HRQOL. Although this is a positive improvement, there was no change in the other subcategories (i.e., physically unhealthy days, mentally unhealthy days, and activity-limited days). However, the overall number of unhealthy days among this population at baseline was already quite low (with less than 3 days per month, on average, across the three categories at baseline). Thus, the possibility to observe significant improvement was somewhat limited. It is also possible that the intensity or duration of the program was inadequate to elicit change in the other categories. Further studies should include program sessions lasting longer than ten weeks as well as aim to conduct follow-up with participants to examine the durability of benefits.
It is important to note that the present study was limited by the pre-post design; a randomized controlled intervention trial would be preferred but was not possible. Also, there are more robust measures for assessing behavior (e.g., accelerometry, as previously mentioned) as well as additional psychosocial measures that could have been added. However, considerations related to cost as well as the content and length of the questionnaires were critical components of feasibility in the community study. Despite these limitations, the present study makes important contributions to the literature in the area of positive psychosocial improvements, such as body image perceptions, as well as physical activity behavior change and attitudes among aging women. It also lends further support about the feasibility of community-based exercise program implementation and outcome evaluation. Perhaps most important, more than 340 women from nine rural counties in Montana were included in the research—a group of individuals who are inadequately represented in the existing literature.
Access to safe and affordable physical activity opportunities are greatly needed in rural communities, and aging women remain one of the most sedentary segments of society. Thus, targeted, evidence-based community exercise programs, which include key social support elements, are free or very low cost, and are feasibly implemented in rural areas (Seguin et al., 2008) hold great promise for improving multiple dimensions of physical, emotional, and mental health among a population with great need that is commonly underserved and understudied. The Family and Consumer Sciences program area of Extension is an ideal organization to implement community-based strength-training programs, such as the Strong Women Program.
Acknowledgments
The authors would like to acknowledge the following Montana State University Extension county agents for their contributions to the research and outreach project reported here: Tara Andrews, Denise Seilstad, Bernie Mason, Jane Wolery, Barbara Andreozzi, Judy Johnson, Alice Burchak, Mary Anne Keyes, Katelyn Andersen, and Jennifer Wells. These Extension professionals provide the skills, experience, and passion for promoting the health of rural women.
References
Ahmed, C., Hilton, W., & Pituch, K. (2002). Relations of strength training to body image among a sample of female university students. Journal of Strength & Conditioning Research, 16(4), 645-648.
Allender, S., Cowburn, G., & Foster, C. (2006). Understanding participation in sport and physical activity among children and adults: a review of qualitative studies. Health Education Research, 21(6), 826-835. doi: cyl06310.1093/her/cyl063
Andresen, E. M., Fouts, B. S., Romeis, J. C., & Brownson, C. A. (1999). Performance of health-related quality-of-life instruments in a spinal cord injured population. Archives of Physical Medicine and Rehabilitation, 80(8), 877-884.
Branch, L. G. (1985). Health practices and incident disability among the elderly. American Journal of Public Health, 75(12), 1436-1439.
Brown, D. W., Balluz, L. S., Heath, G. W., Moriarty, D. G., Ford, E. S., Giles, W. H., & Mokdad, A. H. (2003). Associations between recommended levels of physical activity and health-related quality of life. Findings from the 2001 Behavioral Risk Factor Surveillance System (BRFSS) survey. Preventive Medicine, 37(5), 520-528.
Brown, D. W., Brown, D. R., Heath, G. W., Balluz, L., Giles, W. H., Ford, E. S., & Mokdad, A. H. (2004). Associations between physical activity dose and health-related quality of life. Medicine and Science in Sports and Exercise, 36(5), 890-896.
Brown, T. A., Cash, T. F., & Mikulka, P. J. (1990). Attitudinal body-image assessment: factor analysis of the Body-Self Relations Questionnaire. Journal of Personality Assessment, 55(1-2), 135-144.
Campbell, A., & Hausenblas, H. A. (2009). Effects of exercise interventions on body image: a meta-analysis. Journal of Health Psychology, 14(6), 780-793. doi: 14/6/78010.1177/1359105309338977
Cardello, A., Winterhalter, C., & Schutz, H. (2003). Predicting the handle and comfort of military clothing fabrics from sensory and instrumental data: development and application of new psychophysical methods. Textile Research Journal, 73, 221.
Caruso, C. M., & Gill, D. L. (1992). Strengthening physical self-perceptions through exercise. The Journal of Sports Medicine and Physical Fitness, 32(4), 416-427.
Centers for Disease Control and Prevention (CDC). (2000). Measuring healthy days: population assessment of health-related quality of life. (2000). US Department of Health and Human Services, CDC. Retrieved from: http://www.cdc.gov/hrqol/monograph.htm
Duncan, M. J., Al-Nakeeb, Y., & Nevill, A. M. (2009). Effects of a 6-week circuit training intervention on body esteem and body mass index in British primary school children. Body Image, 6(3), 216-220. doi: S1740-1445(09)00036-910.1016/j.bodyim.2009.04.003
Fitzgerald, N., & Spaccarotella, K. (2009). Barriers to a healthy lifestyle: Fom individuals to public policy—An ecological perspective Journal of Extension [On-line], 47(1) Article 1FEA3. Available at: http://www.joe.org/joe/2009february/a3.php
Green, M. W., & Rogers, P. J. (1995). Impaired cognitive functioning during spontaneous dieting. Psychological Medicine, 25(5), 1003-1010.
Grogan, S., Fry, G., Gough, B., & Conner, M. (2009). Smoking to stay thin or giving up to save face? Young men and women talk about appearance concerns and smoking. British Journal of Health Psychology, 14(Pt 1), 175-186. doi: 30160710.1348/135910708X327617
Haas, C. F., Champion, A., & Secor, D. (2008). Motivating factors for seeking cosmetic surgery: a synthesis of the literature. Plastic Surgical Nursing, 28(4), 177-182. doi: 10.1097/PSN.0b013e31818ea83200006527-200810000-00006
Haskell, W. L., Lee, I. M., Pate, R. R., Powell, K. E., Blair, S. N., Franklin, B. A., Macera, C. A., Heath, G. W., Thompson, P. D., & Bauman, A. (2007). Physical activity and public health: updated recommendation for adults from the American College of Sports Medicine and the American Heart Association. Medicine and Science in Sports and Exercise, 39(8), 1423-1434.
Hausenblas, H. A., Janelle, C. M., Gardner, R. E., & Hagan, A. L. (2003). Affective responses of high and low body satisfied men to viewing physique slides. Eating Disorders, 11(2), 101-113. doi: 0CJ2VXQPCLTXKJP010.1080/10640260390199299
He, X. Z., & Baker, D. W. (2004). Body mass index, physical activity, and the risk of decline in overall health and physical functioning in late middle age. American Journal of Public Health, 94(9), 1567-1573.
Kang, M., & Russ, R. (2009). Activities that promote wellness for older adults in rural communities. Journal of Extension [On-line], 47(5) Article 5RIB2. Available at: http://www.joe.org/joe/2009october/rb2.php
Kruger, T., Murray, D., & Zanjani, F. (2011). Rural community members' perspectives on mental health and aging: an ecological approach to interpreting and applying focus group results. Journal of Extension [On-line], 49(2) Article 2FEA7. Available at: http://www.joe.org/joe/2011april/a7.php
Lubans, D. R., & Cliff, D. P. (2011). Muscular fitness, body composition and physical self-perception in adolescents. Journal of Science and Medicine in Sport, 14(3), 216-221. doi: S1440-2440(10)00202-110.1016/j.jsams.2010.10.003
Lubans, D. R., Sheaman, C., & Callister, R. (2010). Exercise adherence and intervention effects of two school-based resistance training programs for adolescents. Preventive Medicine, 50(1-2), 56-62. doi: S0091-7435(09)00602-110.1016/j.ypmed.2009.12.003
Martin Ginis, K. A., Eng, J. J., Arbour, K. P., Hartman, J. W., & Phillips, S. M. (2005). Mind over muscle? Sex differences in the relationship between body image change and subjective and objective physical changes following a 12-week strength-training program. Body Image, 2(4), 363-372. doi: S1740-1445(05)00073-210.1016/j.bodyim.2005.08.003
McLean, S. A., Paxton, S. J., & Wertheim, E. H. (2010). Factors associated with body dissatisfaction and disordered eating in women in midlife. International Journal of Eating Disorders, 43(6), 527-536. doi: 10.1002/eat.20737
Moriarty, D. G., Zack, M. M., & Kobau, R. (2003). The Centers for Disease Control and Prevention's Healthy Days Measures - population tracking of perceived physical and mental health over time. Health and Quality of Life Outcomes, 1, 37.
Nelson, M. E., Rejeski, W. J., Blair, S. N., Duncan, P. W., Judge, J. O., King, A. C., Macera, C. A., Castaneda-Sceppa, C. (2007). Physical activity and public health in older adults: recommendation from the American College of Sports Medicine and the American Heart Association. Medicine and Science in Sports and Exercise, 39(8), 1435-1445.
Ounpuu, S., Krueger, P., Vermeulen, M., & Chambers, L. (2000). Using the U.S. Behavior Risk Factor Surveillance System's health related quality of life survey tool in a Canadian city. Canadian Journal of Public Health, 91(1), 67-72.
Peat, C. M., Peyerl, N. L., & Muehlenkamp, J. J. (2008). Body image and eating disorders in older adults: a review. The Journal of General Psychology, 135(4), 343-358. doi: 10.3200/GENP.135.4.343-358
Pelican, S., Paul, L., Raidl, M., Gossett, L., & Lanting, R. (2006). Steps to a New You helps participants change lifestyle habits related to food, physical activity, and body image. Journal of Nutrition Education and Behavior, 38(4), S34.
Penedo, F. J., & Dahn, J. R. (2005). Exercise and well-being: a review of mental and physical health benefits associated with physical activity. Current Opinion in Psychiatry, 18(2), 189-193.
Pratt, C., & Bowman, S. (2008). Principles of effective behavior change: application to Extension family educational programming. Journal of Extension [On-line], 46(5) Article 5FEA2. Available at: http://www.joe.org/joe/2008october/a2.php
Reel, J. J., Greenleaf, C., Baker, W. K., Aragon, S., Bishop, D., Cachaper, C., Handwerk, P., Locicero, J., Rathburn, L., Reid, W. K., & Hattie, J. (2007). Relations of body concerns and exercise behavior: a meta-analysis. Psychological Reports, 101(3 Pt 1), 927-942.
Seguin, R. A., Economos, C. D., Hyatt, R., Palombo, R., Reed, P. N., & Nelson, M. E. (2008). Design and national dissemination of the StrongWomen Community Strength Training Program. Preventing Chronic Disease, 5(1), A25.
Seguin, R. A., Heidkamp-Young, E., Kuder, J., & Nelson, M. E. (2012). Improved physical fitness among older female participants in a nationally disseminated, community-based exercise program. Health Education & Behavior, 39(2):183-90.
Shaw, J. M., Ebbeck, V., & Snow, C. M. (2000). Body composition and physical self-concept in older women. Journal of Women & Aging, 12(3-4), 59-75. doi: 10.1300/J074v12n03_05
Singh, N. A., Clements, K. M., & Fiatarone, M. A. (1997a). A randomized controlled trial of progressive resistance training in depressed elders. Journal of Gerontology: Medical Sciences, 52(1), M27-35.
Singh, N. A., Clements, K. M., & Fiatarone, M. A. (1997b). A randomized controlled trial of the effect of exercise on sleep. Sleep, 20(2), 95-101.
Slevec, J. H., & Tiggemann, M. (2011). Predictors of body dissatisfaction and disordered eating in middle-aged women. Clinical Psychology Review, 31(4), 515-524. doi: 10.1016/j.cpr.2010.12.002 S0272-7358(10)00196-0
Speck, R. M., Gross, C. R., Hormes, J. M., Ahmed, R. L., Lytle, L. A., Hwang, W. T., & Schmitz, K. H. (2010). Changes in the Body Image and Relationship Scale following a one-year strength training trial for breast cancer survivors with or at risk for lymphedema. Breast Cancer Research and Treatment, 121(2), 421-430. doi: 10.1007/s10549-009-0550-7
Stephenson, L. (2012). My community, my voice: Rural older adults speak through photography. Journal of Extension [On-line], 50 (1) Article 1FEA7. Available at: http://www.joe.org/joe/2012february/a7.php
Thompson, J., Heinberg, L., Altabe, M., & Tantleff-Dunn, S. (1999). Exacting beauty: theory, assessment, and treatment of body image disturbance. Washington DC: American Psychological Association.
Tiggemann, M. (2004). Body image across the adult life span: stability and change. Body Image, 1(1), 29-41.
Tucker, L. A., & Mortell, R. (1993). Comparison of the effects of walking and weight training programs on body image in middle-aged women: an experimental study. American Journal of Health Promotion, 8(1), 34-42.
U.S. Census Bureau. (2009). Annual estimates of the population for counties of Montana: April 1, 2000 to July 1, 2008. U.S. Census Bureau, Population Division. Retrieved from: http://ceic.mt.gov/graphics/Data_Maps/Co_density_08.pdf
USDA Economic Research Service. Retrieved from: http://www.ers.usda.gov/StateFacts/MT.htm
von Bonsdorff, M., & Rantanen, T. (2011). Progression of functional limitations in relation to physical activity: a life course approach. European Review of Aging and Physical Activity, 8(1), 23-30.
Wilcox, S., Castro, C., King, A. C., Housemann, R., & Brownson, R. C. (2000). Determinants of leisure time physical activity in rural compared with urban older and ethnically diverse women in the United States. Journal of Epidemiology and Community Health, 54(9), 667-672.
Young, D., Weinert, C., & Spring, A. (2012). Home on the range—Health literacy, rural elderly, well-being. Journal of Extension [On-line], 50(3) Article 3FEA2. Available at: http://www.joe.org/joe/2012june/a2.php