April 2009
|
April 2009 // Volume 47 // Number 2 // Research In Brief // v47-2rb3



The Resilience Factor: What Extension Can Learn from Adolescents Coping with Parental Cancer
Abstract
Using a developmental systems framework and grounded theory methods, the study reported here describes the psychosocial experiences of late adolescents coping with parental cancer. Results suggest three primary psychosocial developmental influences, including multilevel influences, coping strategies to maintain control, and responses to uncertainty and anticipatory grief. Identity and intimacy were the two most salient psychosocial tasks. The central unifying concept of resilience was the primary psychosocial developmental outcome that resulted from coping with parental cancer during late adolescence. This finding illuminates the need for Extension to expand its focus on positive outcomes that can result from coping with life crises during adolescence.
Introduction
Adults with life-threatening illnesses are living longer than ever before thanks to modern medical interventions. Prolonged life is generally viewed as a positive change, often accompanied by improved quality of end-of-life care for patients and their families. However, extending the terminal phase of a disease can place a heavier burden on family members with caretaking and financial responsibilities. This extended terminal phase has important implications for the development of adolescents whose parents have been diagnosed with terminal cancer.
In our work with at-risk audiences through Extension, we need to consider the home lives of adolescents and young adults we serve. This reflects a paradigm shift in our organization toward a systemic or ecological framework where multiple contexts must be considered in our work with youth. The programs and skills we teach young people may have minimal impact among those coping with the acute stress associated with life-threatening illness in their families if we do not address the issues they are facing.
We need to be comfortable talking about illness and death in families and be prepared to understand and support adolescents who are coping with these experiences. We also need to listen to the needs and experiences of these young people to develop more effective prevention efforts through Extension that are geared toward adolescents facing all kinds of family crises. We will then be better prepared to reach out to those who can benefit the most from the services we offer.
The purpose of the study reported here was to develop grounded theory on the psychosocial experiences of late adolescents coping with parental cancer. This research was guided by a developmental systems perspective, which views adolescents as developing within an interdependent family system and larger ecological context. The research questions were (a) What are the particular psychosocial developmental impacts or experiences that result from coping with parental cancer during late adolescence? and (b) What are the most salient psychosocial developmental influences identified by late adolescents who are coping with parental cancer? The psychosocial tasks of adolescence explored in the study were achievement, autonomy, identity, intimacy, and sexuality (Hill, 1980). The findings are instructive for Extension professionals who work with adolescents and families coping with illness, death, or other major life crises.
Background
The literature pertaining to adolescent psychosocial experiences of coping with parental cancer can be divided into three major areas of study:
- Adolescent grief and bereavement (Adams et al., 1999; Balk, 1996, 1997, 1998, 2001; Christ, 2000; Dowdney, 2000; Marwit & Carusa, 1998; Morin & Welsh, 1996; Siegel et al., 1992; Thompson et al., 1998; Tyson-Rawson, 1996; Van Epps, Opie, & Goodwin, 1997);
- Anticipatory grief and terminal illness (Berezin, 1977; Kowalski, 1986; Lund, 1989; Moss, Moss, & Hansson, 2001; Parkes, 1975; Peterson & Rafuls, 1998; Rando, 1997); and
- Psychosocial development and death (Adams, 1997; Balk, 1996, 1998, 2000; Carter & McGoldrick, 1999; Corr, 2000; DeBaryshe, Patterson, & Capaldi, 1993; Douvan & Adelson, 1966; Fleming & Balmer, 1996; Goosens & Phinney, 1996; Grotevant, 1998; Hill, 1980; Horton, 1998; Ingersoll, 1998; Kandt, 1994; Klass, 1993; Lerner, 2002; Parkes, 1993; Schultz, 1999; Shapiro, 1994; Silverman & Worden, 1993; Steinberg, 1996; Tyson-Rawson, 1996; Worden, 1996; Yoder, 2000).
This literature base has not yet filled in many of the gaps for answering the research questions in the study reported here. Outcomes have been mixed, developmental stages have not been explored separately, and the influence of the larger environment remains largely unexplored. In fact, this literature suggests a need to examine the larger environmental context to more fully understand the impact that parental illness and death has on adolescents' development and attitudes toward the future. Studies also indicate a need to examine risk factors, protective factors, and systemic influences identified by adolescents who are coping with parental cancer.
Most specific to the study, the literature on anticipatory grief and terminal illness points to the utility of studying the time period prior to parental death and to examining the impacts and meanings parental illness has for adolescents. The study reported here attempted to fill these gaps by developing grounded theory on the psychosocial experiences of late adolescents at the interface of coping with parental cancer.
Methods
The sample for the qualitative study consisted of five males and three females. (See Table 1 for participant characteristics>) The procedures for data collection and analysis were modeled after grounded theory, a general method of comparative analysis that uses a systematically applied set of methods to generate inductive theory about a substantive area (Glaser, 1992). Data were collected through one in-depth, qualitative interview with each of the eight participants.
| Nickname | Gender | Age at Interview | Age at Diagnosis | Diagnosis of Parent | Gender of Parent | Status of Parent |
| Tai | M | 20 | 19 | Pancreatic | M | Living |
| Dave | M | 20 | 20 | Breast | F | Living |
| Shawn | M | 18 | 16 | AML (Leukemia) | F | Deceased |
| Pierre | M | 19 | 19 | Esophageal | M | Living |
| Victoria | F | 21 | 16 | Stomach | F | Deceased |
| Elayne | F | 51 | 18 | Bone Marrow | M | Deceased |
| Nat | F | 28 | 16 | Blood | M | Deceased |
| Narsky | M | 21 | 11 | Mantle Cell Lymphoma | M | Deceased |
The interviews consisted of 13 open-ended questions about coping with parental cancer during late adolescence designed to gain a better understanding of psychosocial developmental experiences and impacts. Information gathered in the interviews included positive and negative experiences encountered during the illness, most and least helpful things about self and others, fears and concerns resulting from the diagnosis and illness, psychosocial tasks encountered as a result of having a parent with cancer, negative and positive impacts of going through this experience, and familial and systems information.
These interviews ranged from 1 to 3 hours in length with each participant. Interviews were all audiotape. Analysis of the data began after the first interview was transcribed and continued throughout the data collection process. This type of analysis is called the "constant comparative method" (Glaser & Strauss, 1967), an inductive form of analysis where each new interview was compared to categories that had emerged from previous interviews. Nvivo™ qualitative data management software was used to facilitate data analysis. Ultimately, nine overall categories containing 30 codes were generated. Selective coding was then used to validate the relationships between the codes and categories as well as the interrelationships between categories and to develop the final grounded theory and developmental systems model (Figure 1).
Results
Research Question 1: What Are the Most Important Psychosocial Developmental Influences Identified by Late Adolescents Who Are Coping with Parental Cancer?
Study participants identified three primary psychosocial developmental influences. The first was multilevel influences, which included individual level influences of perceived role in the family system and personal theories on the experience of parental cancer that were related back to autonomy and identity; familial level influences of attachments, communication, family dynamics, prior losses, and family roles, which were related back to intimacy, autonomy, and identity; and extrafamilial level influences of others' ignorance, support, and understanding, which were related back to intimacy. There were 10 codes containing 41 themes on three levels of influence (Table 2) that participants perceived as influencing their psychosocial experience from the time of a parent's cancer diagnosis up to and beyond a parent's death.
| Subcategories | Codes | Prominent Themes |
| Individual | Perceived role in family | Birth order, life-long identity, evolved identity, identifying with ill parent, what identity did not or could have evolved into, level of autonomy |
| Theories on the experience of parental cancer | Self as normal, self as different, dichotomies, culture and society | |
| Participant Quote: "He was diagnosed with cancer as soon as I leave for school....Something like this is happening at the time where we need to be moving into the house to help out. It kind of seems like the exact opposite of what needs to be going on." - Tai | ||
| Familial | Attachments and bonds | Bond with ill parent, bond with non-ill parent, increase in closeness, impact of illness on attachment |
| Family communication | Communication channels, increase in communication, future orientation, avoidance | |
| Family dynamics | Addiction, cutoffs, secrets, suppression of emotion, triangles | |
| Family roles | Informant, filling in, primary role of ill parent, non-ill parent as helpful or not helpful, sibling roles | |
| Prior losses | Grandparents, divorce | |
| Participant Quote: "It forced me to create my identity, first in coming out with my sexuality, second with just, forcing, my stepdad and my brother wanted me to automatically take my mother's position, take her role...I rejected that because I'm a sister, I'm a daughter. I'm not a mother and I realized that I needed to detach myself away from that a little bit...become my own person." - Victoria | ||
| Extrafamilial | Ignorance | Insensitivity, avoidance and forgetting, don't know what it's like, apologies, sympathy |
| Support | Openness, offering help, being there | |
| Understanding | Comfort, relating | |
| Participant Quote: "You just need to be there...it's okay to be worrying about something other than their parent, that they do have their own concerns and their own life doesn't stop because of what's going on....Just be there to do whatever needs to be done." - Elayne | ||
The second area of influence on psychosocial development was coping strategies to maintain control. Coping strategies were a route for accomplishing or hindering the psychosocial tasks of late adolescence in the midst of their family crises. Analyses resulted in 11 codes containing 27 themes. These codes were organized into three domains of coping, including appraisal-focused strategies, which were tied to identity; problem-focused strategies, which were connected to all five psychosocial developmental tasks; and emotion-focused strategies, which were tied to achievement, identity, intimacy, and sexuality (Table 3). These domains came from existing research on coping with life crises (Moos & Schaefer, 1986) due to a close fit with participants' terms. A common thread that ran between these codes and themes was maintaining balance and control. This was viewed as a crucial aspect of facing a crisis like parental cancer. The overwhelming nature of the crisis led some respondents to lose a sense of control over their lives.
| Subcategories | Codes | Prominent Themes |
| Appraisal Focused | Denial | Dodging, false optimism, naivety |
| Journaling | NA | |
| Negative thinking | Fatalism, giving up, hopelessness, self-pity | |
| Theorizing | Causes, culture, gender, getting over it | |
| Participant Quote: "The main thing that got me through it was myself...remembering the little things that happen over a week or that happened over the past year, and just talking them out to yourself and rationalizing them...what happened as far as your parent dying or going to the hospital....it's the hardest thing for somebody to do, make a positive out of a negative."-Narsky | ||
| Problem Focused | Multiple stresses | Juggling act |
| Knowledge seeking | NA | |
| Priority Changes | Priority reversal, quality time, re-assessing romantic relationships | |
| Participant Quote: "[School work] was hopeless and seemed a chore because it was my very first semester, my very first year....I'm sitting there studying for finals, I have all this crap going on with the family, and I'm sitting around looking at my physics notes thinking, 'What the crap is this?' I have no idea what I'm looking at." - Pierre | ||
| Emotion Focused | Escape | Drugs, exercise/sports, sex, staying busy, studying |
| Fantasizing | Release, substitutions, support, turning back time | |
| Guilt | Not being there, self-absorption | |
| Humor | Breaking the ice | |
| Participant Quote: "When she was first diagnosed, I played basketball. I was really into it, so I guess that helped me a lot. I kept busy like that, and I do it to this day. I just think that if I keep being busy that I can't dwell on things." - Victoria | ||
The third area of influence on psychosocial development was responding to uncertainty and anticipatory grief. Uncertainty was an important factor in understanding participants' responses to illness and dying because the chronic stress from uncertainty left them feeling like they had no control. One participant noted that uncertainty was the most negative part of the whole experience due to the "constant fact of not knowing what's going to happen." Analyses resulted in 10 codes containing 25 themes. These codes were organized into three subcategories (Table 4), including triggers, which were connected to identity; concerns for the future, which were connected to autonomy, identity, intimacy, and sexuality; and meaning making, which was connected to achievement, autonomy, and identity.
| Subcategories | Codes | Prominent Themes |
| Triggers | Changes in ill parent | Decline, remission, what is wrong? |
| Helplessness | Feeling incapacitated, no control, inevitability of death | |
| Suddenness | Emotional reactions, no time to prepare | |
| Participant Quote: "[My father] had always been such a big man. I can remember looking at his hands, because they'd always been huge, but I kept thinking how small they looked, and I just couldn't go back [to the hospital]." - Elayne | ||
| Concerns for Future | Fears for self | Filling the void, getting cancer, transference of fear |
| Future losses | Developmental milestones, drifting apart, other deaths | |
| Post-death changes | Reestablishing routines or normalcy, role renegotiation | |
| Participant Quote: "I don't know that I'm ever gonna be able to share the same type of relationship with anyone I had with my mom...it was just totally unique, kind of awesome, connection that we had, and I don't know that it's replaceable." - Shawn | ||
| Meaning Making | Advice to others | Perseverance, seizing the moment, self-reliance |
| Closure | Barriers, peace of mind | |
| Faith | Afterlife, putting things in God's hands | |
| Legacy | Carrying on the torch, desire to help others | |
| Participant Quote: "As time goes on, the positives begin to outweigh any of the negatives. That's what you have to focus on." - Dave | ||
Research Question 2: What Are the Particular Psychosocial Developmental Experiences or Impacts That Result from Coping with Parental Cancer During Late Adolescence?
The central unifying concept of resilience was the primary psychosocial developmental experience and impact that resulted from coping with parental cancer during late adolescence. Resilience is conceptually defined as the ability to stretch or flex in response to pressures and strains, including normative stress from everyday hassles, expected transitions, and stress and trauma from the unexpected (Boss, 2006). Participants believed they had experienced a "fork in the road" where they consciously decided which way they would go.
Nat describe this phenomenon by stating that each person had to decide whether to be "bitter or better." Dave described a pivotal moment where one direction would be "dark, cold, and depressing," and the other was "appreciation and optimism." Victoria saw it as "going one of two ways" when faced with "adversity."
Adolescents can either get "really depressed and fail" or "put all that energy and emotion into succeeding." All participants chose the positive route, which revealed a form of resilience in action as the final grounded theory derived from the study (Figure 1). This conscious choice to take a resilient path seemed to affect all aspects of their psychosocial experience. The resulting maturity they gained then fed back into their individual, familial, and extrafamilial experiences, which enhanced their coping strategies and responses to uncertainty and anticipatory grief, and facilitated further psychosocial development.
This finding supports the notion that more attention needs to be paid to restoration, a positive aspect of development that can occur after parental loss (Balk, 1998; Stroebe & Schut, 1999). The primary difference was that the study reported here targeted the time period prior to a loss. Thus, the concept used to describe this positive development prior to a parent's death was resilience rather than restoration.
Figure 1.
Developmental Systems Model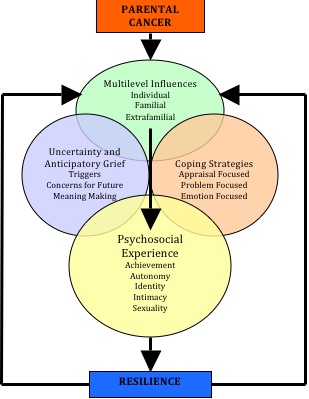
Conclusions & Implications for Extension Professionals
There are five primary implications from this study that Extension professionals can apply to practice (Table 5). These results can serve to enhance understanding of the interplay of multiple risk and protective variables in the presence of traumatic life events and paths toward resilience.
| Recommendation | Translating to Extension Practice |
| Attending to Context |
1) Adolescents do not develop in a vacuum. Practitioners must remember the context of development and help adolescents find ways to navigate through all levels of influence. 2) It is important to work directly with adolescents, but supporting/educating parents provides care for the parents, which indirectly provides care for adolescents, facilitating the development of protective factors. |
| Need for Support |
1) Listening was an important aspect of support for this age group. They want people to communicate honestly with them and keep them in the loop, but mostly need someone to be there to listen. 2) Relating was a second important aspect of support. This age group believed it was crucial to feel like there was someone else that could identify with them. Practitioners can bring people together in a group atmosphere and find ways to connect people who have shared similar experiences in order to allow adolescents to feel understood and less alone while they are coping with a major life crisis. |
| Creative Coping Solutions | 1) Practitioners can help adolescents in finding creative and satisfactory ways to cope, but also be non-judgmental about strategies that have been employed in their attempts to cope. 2) Adolescents need assistance in realizing what they can and cannot control and with letting go of guilt about things they cannot control. 3) Practitioners can help adolescents derive meaning out of their experiences and put it to positive use for themselves and others. |
| Holistic/Develop- mentally Grounded Practice | 1) Identity and intimacy were the most heavily influenced psychosocial tasks in this study. This can serve as a starting point for programs/ support groups that assist this audience. The other tasks can then be woven into discussions on identity and intimacy. 2) This study revealed the importance of developmental grounding. Practitioners can use developmental grounding in their efforts to help adolescents who are coping with major life crises because it offers a lens for creating some order out of a complex crisis. |
| Risk and Protective Factors | 1) Practitioners can uncover the protective factors present in adolescents' lives to help them bolster existing factors and to develop new protective factors they do not yet have. 2) Practitioners can help adolescents become aware of risk factors in their lives and assist them to reduce these risks. Practitioners can also reframe risk factors as opportunities for growth/skill development that can become protective factors by gaining strength out of adversity. |
Terminal illness can require renegotiation of individual and family development and processes as family members cope with constant uncertainty, multiple stresses, and shifts in communication, roles, and priorities. Understanding the unique experiences adolescents face when confronted with parental illness and death can lead to developmentally and contextually appropriate interventions and resources. The resiliency factors used by these adolescents to negotiate developmental tasks in the midst of coping with a major family crisis may also be informative for Extension professionals when working more generally with issues of death and dying or with family crises.
In conclusion, the study was exploratory, and the conclusions that can be drawn from it are limited, but it does suggest some key issues for Extension professionals to consider when working with this population. These findings help to build a knowledge base for preventing negative short- and long-term outcomes from traumatic life events. Extension professionals cannot prevent an adolescent from experiencing a crisis, but can help to bolster protective factors and make adolescents aware of risk factors in their lives. This awareness can go a long way in learning how to cope with a major crisis.
Extension professionals who are working with at-risk adolescents should not make assumptions that only negative outcomes are possible or that youth in all developmental stages of adolescence experience parental illness uniformly. Instead, future research, theoretical development, and practice should focus on positive outcomes that can result from the experience (Balk, 1998; Stroebe & Schut, 1999; Tyson-Rawson, 1996). Examples of positive outcomes include increased maturity, life skills and competencies gained for coping with future problems, improved confidence, and improved physical and mental health, which can lead to productive contributions as adult members of society. Extension professionals play an important role in developing skills that foster strength through adversity and, accordingly, we can set the stage for improving developmental outcomes for adolescents coping with a major crisis such as parental cancer.
References
Adams, D. W., Corr, C. A., Davies, B., Deveau, E., de Veber, L. L., Martinson, I. M. et al. (1999). Children, adolescents, and death: Myths, realities, and challenges. Death Studies, 23, 443-464.
Adams, G. R. (1997). Identity: A brief critique of a cybernetic model. Journal of Adolescent Research, 12, 358-362.
Balk, D. E. (1996). Models for understanding adolescent coping with bereavement. Death Studies, 20, 367-387.
Balk, D. E. (1997). Death, bereavement, and college students: A descriptive analysis. Mortality, 2, 207-221.
Balk, D. E. (1998). Psychological development during four years of bereavement: A longitudinal case study. Death Studies, 22, 23-36.
Balk, D. E. (2000). Adolescents, grief, and loss. In K. J. Doka (Ed.), Living with grief: Children, adolescents, and loss (pp. 35-49). Washington, DC: Hospice Foundation of America.
Balk, D. E. (2001). College student bereavement, scholarship, and the university: A call for university engagement. Death Studies, 25, 67-84.
Berezin, M. A. (1977). Partial grief for the aged and their families. In E. M. Pattison (Ed.), The experience of dying (pp. 279-286). Englewood Cliffs, NJ: Prentice Hall.
Boss, P. (2006). Loss, trauma, and resilience: Therapeutic work with ambiguous loss. New York: W.W. Norton and Company.
Carter, B., & McGoldrick, M. (Eds.). (1999). The expanded family life cycle: Individual, family, and social perspectives (3rd ed.). Needham Heights, MA: Allyn and Bacon.
Christ, G. H. (2000). Healing children's grief: Surviving a parent's death from cancer. New York: Oxford University Press.
Corr, C. A. (2000). What do we know about grieving children and adolescents? In K. J. Doka (Ed.), Living with grief: Children, adolescents, and loss (pp. 21-32). Washington, DC: Hospice Foundation of America.
DeBaryshe, K., Patterson, G., & Capaldi, D. (1993). A performance model for academic achievement in early adolescent boys. Developmental Psychology, 29, 795-804.
Douvan, E., & Adelson, J. (1966). The adolescent experience. New York: Wiley.
Dowdney, L. (2000). Childhood bereavement following parental death. Journal of Child Psychology and Psychiatry, 41, 819-830.
Fleming, S., & Balmer, L. (1996). Bereavement in adolescence. In C. A. Corr & D. E. Balk (Eds.), Handbook of adolescent death and bereavement (pp. 139 - 154). New York: Springer Publishing.
Glaser, B., & Strauss, A. L. (1967). The discovery of grounded theory: Strategies for qualitative research. Chicago: Aldine.
Goosens, L., & Phinney, J. S. (1996). Identity, context, and development. Journal of Adolescence, 19, 491-496.
Grotevant, H. (1998). Adolescent development in family contexts. In W. Damon & N. Eisenberg (Eds.), Handbook of child psychology: Vol. 3. Social, emotional and personality development (pp. 1097-1149). New York: Wiley.
Hersh, S. P. (1997). Death from the cancers. In K. J. Doka (Ed.), Living with grief: When illness is prolonged. Washington, DC: Hospice Foundation of America.
Hill, J. P. (1980). Understanding early adolescence: A framework. Chapel Hill, NC: University of North Carolina Center for Early Adolescence.
Horton, D. A. (1998). Adolescent daughters and the impact and meaning of the loss of their mothers to breast cancer. Dissertation Abstracts International - Section B: The Sciences and Engineering, 59(5-B).
Ingersoll, G. M. (1998). Normal adolescence. Bloomington, IN: Center for Adolescent Studies.
Kandt, V. E. (1994). Adolescent bereavement: Turning a fragile time into acceptance and peace. School Counselor, 41, 203-212.
Klass, D. (1993). Solace and immortality: Bereaved parents' continuing bond with their children. Death Studies, 17, 343-368.
Kowalski, N. C. (1986). Anticipating the death of an elderly parent. In T. A. Rando (Ed.), Loss and anticipatory grief (pp. 187-199). Lexington, MA: Lexington Books.
Lerner, R. M. (2002). Adolescence: Development, diversity, context, and application. Upper Saddle River, NJ: Pearson Education.
Lund, D. A. (1989). Conclusions about bereavement in later life and implications for interventions and future research. In D. A. Lund (Ed.), Older bereaved spouses (pp. 217-231). New York: Hemisphere.
Marwit, S. J., & Carusa, S. S. (1998). Communicated support following loss: Examining the experiences of parental death and parental divorce in adolescence. Death Studies, 22, 237-256.
Moos, R., & Schaefer, J. (1986). Life transitions and crises: A conceptual overview. In R. Moos (Ed.), Coping with life crises: An integrated approach (pp. 1-28). New York: Plenum Press.
Morin, S. M., & Welsh, L. A. (1996). Adolescents' perceptions and experiences of death and grieving. Adolescence, 31, 585-596.
Moss, M. S., Moss, S. Z., & Hansson, R. O. (2001). Bereavement and old age. In M. S. Stroebe, R. O. Hansson, W. Stroebe, & H. Schut (Eds.), Handbook of bereavement research: Consequences, coping, and care (pp. 241-260). Washington, DC: American Psychological Association.
Parkes, C. M. (1975). Bereavement: Studies of grief in adult life. Harmondsworth: Penguin.
Parkes, C. M. (1993). Bereavement as a psychosocial transition: Processes of adaptation to change. In M. S. Stroebe, W. Stroebe, & R. O. Hansson (Eds.), Handbook of bereavement: Theory, research, and intervention (pp. 91-101). New York: Cambridge University Press.
Peterson, S., & Rafuls, S. E. (1998). Receiving the scepter: The generational transitions and impact of parent death on adults. Death Studies, 22, 493-524.
Rando, T. A. (1997). Living and learning the reality of a loved one's dying: Traumatic stress and cognitive processing in anticipatory grief. In K. J. Doka (Ed.), Living with grief: When illness is prolonged. Washington, DC: Hospice Foundation of America.
Schultz, K. (1999). Bereaved children. Canadian Family Physician, 45, 2914-2921.
Shapiro, E. R. (1994). Grief as a family process: A developmental approach to clinical practice. New York: Guilford Press.
Siegel, K., Karus, D., & Raveis, V. (1996). Adjustment of children facing the death of a parent due to cancer. Journal of the American Academy of Child and Adolescent Psychiatry, 35, 442-456.
Siegel, K., Mesagno, F. P., Karus, D., Christ, G., Banks, K., & Moynihan, R. (1992). Psychosocial adjustment of children with a terminally ill parent. Journal of the American Academy of Child and Adolescent Psychiatry, 31, 327-333.
Silverman, P. R., & Worden, J. W. (1993). Children's reactions to the death of a parent. In M. S. Stroebe, W. Stroebe, & R. O. Hansson (Eds.), Handbook of bereavement: Theory, research, and intervention (pp. 300-316). New York: Cambridge University Press.
Steinberg, L. D. (1996). Adolescence (4th ed.). New York: McGraw Hill.
Strauss, A., & Corbin, J. (1990). Basics of qualitative research: Grounded theory procedures and techniques. Newbury Park, CA: Sage Publications.
Strauss, A., & Corbin, J. (1994). Grounded theory methodology. In N. K. Denzin & Y. S. Lincoln (Eds.), Handbook of qualitative research (pp. 273-285). Thousand Oaks, CA: Sage Publications.
Strauss, A., & Corbin, J. (1998). Basics of qualitative research: Techniques and procedures for developing grounded theory. Thousand Oaks, CA: Sage Publications.
Stroebe, M., & Schut, H. (1999). The dual process model of coping with bereavement: Rationale and description. Death Studies, 23, 197-224.
Thompson, M. P., Kaslow, N. J., Kingree, J. B., King, M., Bryant, L., & Rey, M. (1998). Psychological symptomatology following parental death in a predominantly minority sample of children and adolescents. Journal of Clinical Child Psychology, 27, 434-441.
Tyson-Rawson, K. (1996). Adolescent responses to the death of a parent. In C. A. Corr & D. E. Balk (Eds.), Handbook of adolescent death and bereavement (pp. 155-172). New York: Springer.
Tyson-Rawson, K. (1996). Relationship and heritage: Manifestations of ongoing attachment following father death. In D. Klass, P. R. Silverman, & S. L. Nickman, (Eds.), Continuing bonds: New understandings of grief (pp. 125-145). New York: Taylor & Francis.
Worden, J. W. (1996). Children and grief: When a parent dies. New York: Guilford.
Yoder, A. E. (2000). Barriers to ego identity status formation: a contextual qualification of Marcia's identity status paradigm. Journal of Adolescence, 23, 95-106.